
The Heart Disease Blind Spot: A Comprehensive Guide to Cardiovascular Health for Women 18–39
Why Your Twenties and Thirties Are the Decades That Decide Your Heart’s Future
Most people think heart disease only affects older men.
This surprising truth: it's the number one killer of women, even in their twenties and thirties. Your estrogen offers some protection, but silent damage starts building decades before symptoms appear. Many doctors miss early warning signs in young women.
Your heart's future depends on what you do right now. Standard cholesterol tests miss the most important risk factors for women your age. You need specific blood markers that actually predict heart problems. Small changes in your twenties can prevent major problems in your fifties and beyond.
Ask for ApoB and Lp(a) tests, not just basic cholesterol panels. Take 2-3 grams daily of EPA/DHA omega-3s to fight inflammation. If your homocysteine is above 8 umol/L, add 400-800 mcg methylfolate plus 500-1,000 mcg B12 daily. Do 150 minutes weekly of zone 2 cardio where you can still talk easily. These steps build the foundation for a healthy heart that lasts decades.
- EPA/DHA (Omega-3 Fatty Acids)
- EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) are the two key active components in fish oil that reduce inflammation and support blood vessel health; the article recommends 2-3 grams daily
- Zone 2 Cardio
- Exercise at a steady, moderate pace—like a brisk walk—where you can still hold a conversation
- MTHFR Variant
- A common genetic change that makes it harder for your body to process certain B vitamins, raising homocysteine and heart risk
- Apolipoprotein B
- Apolipoprotein B, the protein component of atherogenic particles. Desirable <90 mg/dL (risk-dependent).
- Homocysteine
- Homocysteine, an amino acid metabolite influenced by B vitamins. elevated levels damage blood vessels and increase cardiovascular and dementia risk.
- C-Reactive Protein (cardiac)
- High-sensitivity C-reactive protein, a liver-produced acute-phase reactant. Independent predictor of heart attack and stroke.
- Atherosclerosis
- The gradual buildup of fatty plaque inside artery walls, which narrows and hardens the arteries over time, restricting blood flow to the heart and other organs.
- 120/80
- A standard measurement representing normal, healthy human blood pressure.
- 130/85
- A blood pressure reading indicating elevated levels or stage 1 hypertension.
- B12
- An essential vitamin crucial for nerve function, red blood cell production, and DNA synthesis.
- CRP
- C-reactive protein is a blood marker indicating the presence of inflammation in the body.
- estrogen
- A primary female sex hormone that helps maintain flexible blood vessels and cardiovascular health.
When you think about heart attacks, the image that probably comes to mind is a middle-aged man clutching his chest. This stereotype is dangerous for women. Heart disease is the leading cause of death for women, outpacing all cancers combined. For women under 40, rates are actually rising, not falling. The problem is worse because young women with cardiac symptoms often get misdiagnosed. Instead of being taken seriously, they may be told it’s just anxiety and sent home.
This happens partly because estrogen does provide some protection for your arteries. It helps keep blood vessels flexible, supports good cholesterol levels, and lowers inflammation. But this “shield” isn’t permanent or perfect. It fluctuates with your menstrual cycle, drops after childbirth, and can become disrupted by chronic stress, PCOS, or hormonal birth control. Crucially, the changes that set the stage for heart disease begin far earlier than menopause. The silent damage that accumulates in your 20s and 30s can determine whether you have a smooth or difficult transition when hormone levels start to drop.
Ignoring heart health until later in life is a costly mistake. The risk is real right now—even if you feel fine. Understanding this blind spot is the first step to protecting your heart for decades to come.
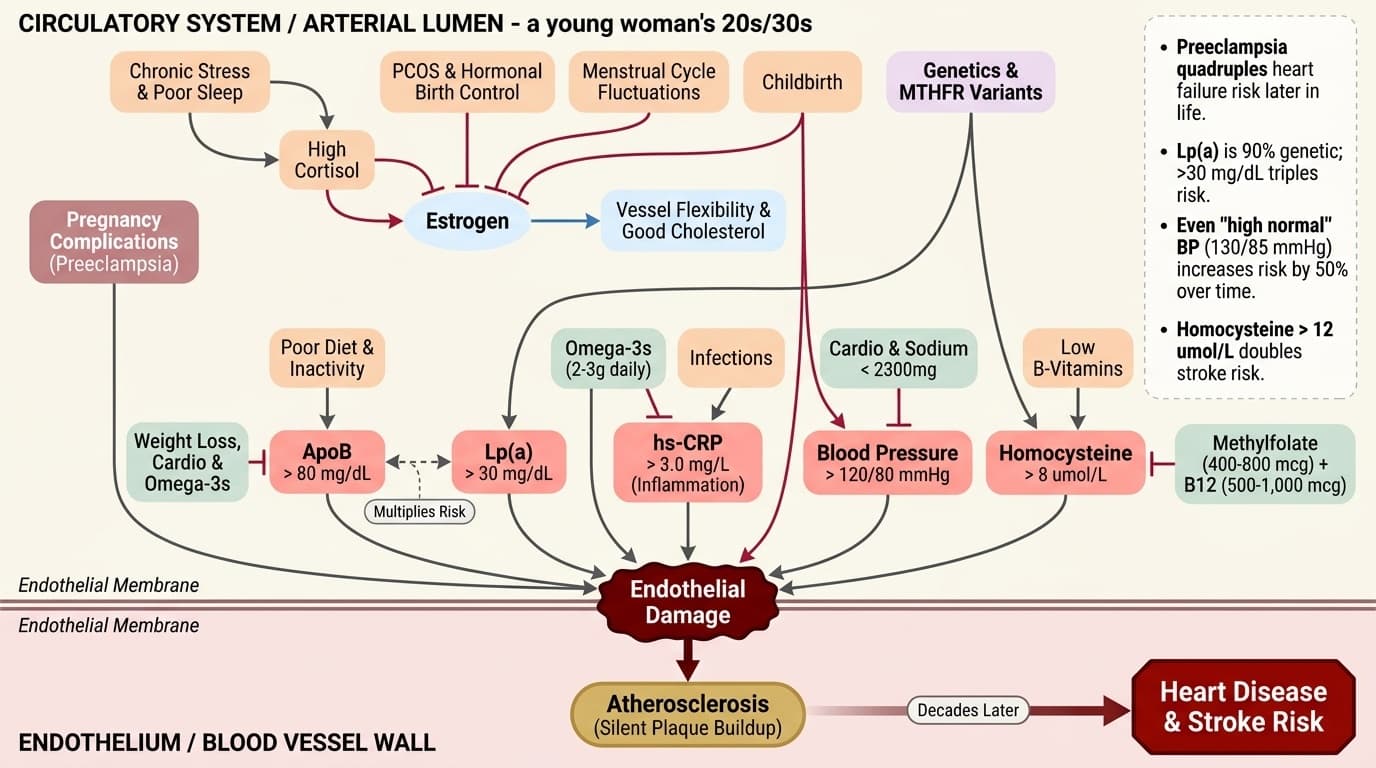
You may not realize it, but atherosclerosis—the gradual buildup of plaque in your arteries—often starts in the teenage years. It’s a slow, silent process. By the time most people notice symptoms, a lot of damage has already been done. For women, certain life events add extra risk. Pregnancy complications like preeclampsia and gestational hypertension are not just one-time problems. Research suggests that preeclampsia, for example, quadruples your risk of heart failure later in life [1]. These conditions act as warning signs, showing that your cardiovascular system is under stress.
Modern life adds its own challenges. Chronic stress from balancing work, family, and caregiving can keep your cortisol levels high. Over time, this damages the walls of your blood vessels and contributes to inflammation. If you have PCOS or use hormonal birth control, your estrogen balance may be disrupted. All these factors can push you toward higher risk, long before traditional symptoms appear.
The critical point: your choices now aren’t just “preventive” in some abstract sense. They are actively building, or eroding, the heart and blood vessels you’ll rely on for the next fifty years. As you move forward, knowing which markers to track and how to interpret them is essential.
Standard cholesterol tests miss the most dangerous risk factors for young women. To truly understand your cardiovascular health, focus on these five markers:
ApoB (Apolipoprotein B) predicts heart risk better than any other single marker. Optimal levels are below 80 mg/dL, though labs often report "normal" up to 100 mg/dL. ApoB counts every particle that can stick in your arteries and cause blockages. Unlike LDL cholesterol, which only measures the cholesterol inside particles, ApoB tells you exactly how many dangerous particles you have. Poor diet and lack of exercise drive ApoB up by 20-40%. Weight loss, regular cardio, and omega-3s can drop it by 15-25% in 8-12 weeks.
Lp(a) (Lipoprotein(a)) reveals your genetic heart risk. Levels above 30 mg/dL triple your risk of heart attack and stroke. This marker is 90% determined by your genes and barely responds to diet or exercise. If your Lp(a) is high, you must aggressively manage other risk factors. When combined with high ApoB, risk multiplies rather than just adds.
hs-CRP (high-sensitivity C-reactive protein) measures inflammation attacking your arteries. Optimal levels are under 1.0 mg/L. Levels above 3.0 mg/L double your heart attack risk. Poor sleep, chronic stress, and infections spike hs-CRP within days. Omega-3s at 2-3 grams daily can lower it by 25% in 4 weeks.
Blood Pressure should stay below 120/80 mmHg. Even "high normal" readings of 130/85 mmHg increase risk by 50% over time. Birth control pills can raise blood pressure by 5-15 points. Regular cardio and cutting sodium to under 2,300mg daily can drop readings by 10-20 points in 2-4 weeks.
Homocysteine damages blood vessel walls directly when above 8 umol/L. Levels above 12 umol/L double stroke risk. Low B-vitamin intake or MTHFR gene variants drive homocysteine up. Methylfolate (400-800 mcg) plus B12 (500-1,000 mcg) daily can cut levels by 30% in 4-8 weeks.
These five markers give you a complete picture of your heart risk and show exactly how your interventions are working.
ApoB and Lp(a) are not always included in standard cholesterol panels, but they offer much more insight into your heart risk than total cholesterol or LDL alone. ApoB is the count of all the particles that can get stuck in your arteries—not just the cholesterol floating around. An optimal ApoB is under 80 mg/dL. If your number is higher, you may have more dangerous particles even if your LDL looks normal. What moves ApoB? Diets high in saturated fat, lack of exercise, and insulin resistance push it up. Weight loss, aerobic exercise (especially zone 2 cardio), and omega-3 supplementation can bring it down. Changes can be seen after 2–3 months of steady effort.
Lp(a) is mostly genetic. If yours is above 30 mg/dL, you can’t lower it much with diet or exercise. But knowing it’s high is crucial: it means you need to pay extra attention to other risk factors, especially ApoB and inflammation. Lp(a) interacts with these other markers, making high levels particularly dangerous if you also have high ApoB or hs-CRP. Some research suggests niacin can lower Lp(a), but it’s not usually recommended due to side effects [2].
For women ages 18–39, these markers are especially important if you have a family history of early heart disease or if you’ve had pregnancy complications. Request these tests specifically—they’re often skipped in routine blood work. Knowing your numbers gives you a real advantage in protecting your future heart health.
Many young women overlook blood pressure and inflammation because they rarely show symptoms early on. Yet these are two of the most powerful predictors of future heart risk.
hs-CRP is your best marker for blood vessel inflammation. An optimal level is below 1.0 mg/L. Elevated hs-CRP can be triggered by poor sleep, high stress, inactivity, or even minor infections. It is also higher in women with conditions such as PCOS or after complicated pregnancies. Studies show that omega-3 supplementation (EPA/DHA, 2–3g daily) lowers hs-CRP and may reduce arterial inflammation within 4 weeks [3].
Blood pressure is another key signal. While many young women have low or normal readings, prehypertension (readings above 120/80 but below 140/90 mmHg) is common and often missed. Birth control pills, chronic stress, and weight gain can all contribute to rising blood pressure. Regular aerobic exercise and lowering salt intake can help bring numbers down within a few weeks. Elevated blood pressure and hs-CRP together are an early warning sign—especially in women with a family history of heart disease.
Tracking these markers regularly gives you an early heads-up. If you see either creeping up, it’s time to take action before structural changes occur in your arteries.
Homocysteine may not be as well known as cholesterol, but it has a direct impact on your blood vessels. When homocysteine levels rise above the optimal range (5–8 umol/L), it can irritate and damage the lining of your arteries, increasing your risk of plaque buildup.
Many women with elevated homocysteine have what’s called an MTHFR variant—a common genetic difference that makes it harder for your body to process B vitamins, especially folate. Low intake of B6, B12, or folate can also drive homocysteine up. The good news: homocysteine responds well to targeted supplementation. Taking methylfolate (the active form of folate) and methylcobalamin (active B12) can lower homocysteine by up to 30% within 1–2 months [4]. The mechanism is simple: these vitamins help your body recycle homocysteine back into methionine, a harmless amino acid.
Why does this matter for women in their reproductive years? High homocysteine is linked not only to heart risk but also to pregnancy complications and fertility issues. If you have a history of miscarriage, preeclampsia, or PCOS, checking your homocysteine and MTHFR status is especially important. Lowering homocysteine reduces both cardiovascular and reproductive risks—two birds with one stone.
When it comes to building a heart-healthy foundation, targeted supplements and lifestyle changes can make a real difference. Here’s what the evidence suggests:
Omega-3 fatty acids (EPA and DHA) have a well-documented impact on lowering triglycerides, reducing inflammation, and improving endothelial function. The recommended dose is 2–3 grams per day of combined EPA/DHA. Look for high-quality, purified fish oil or algal oil capsules. Studies indicate this dose lowers hs-CRP by up to 25% and can reduce triglycerides in 8–12 weeks [5]. Omega-3s work even better when combined with aerobic exercise, amplifying benefits for blood vessel flexibility.
Methylfolate and B12, as discussed earlier, are critical if your homocysteine is high or if you carry MTHFR variants. The optimal intervention is 400–800 mcg of methylfolate and 500–1,000 mcg of methylcobalamin daily. These forms are more bioavailable than standard folic acid or cyanocobalamin, especially in women with MTHFR variants. Supplementing these vitamins lowers homocysteine and supports both heart and reproductive health.
Regular aerobic exercise, especially zone 2 cardio (where you can talk easily), strengthens your heart muscle and improves vascular compliance. Aim for at least 150 minutes per week. Exercise also helps lower ApoB, blood pressure, and inflammation. Synergistically, pairing omega-3s with exercise boosts the anti-inflammatory effect [6].
Each intervention targets a different aspect of heart risk. Using them together creates a powerful, personalized stack for cardiovascular protection.
Women’s heart symptoms can look very different from men’s. Instead of crushing chest pain, you’re more likely to experience jaw pain, nausea, overwhelming fatigue, shortness of breath, or upper back pressure during a cardiac event. These subtle signs are often overlooked, both by patients and healthcare providers.
If you have a family history of early heart disease (before age 55 in male relatives, or before 65 in female relatives), you need to be especially proactive. Take note of blood pressure readings that hover above 130/85 mmHg, especially during or after hormonal birth control use. If you’ve ever had pregnancy complications like preeclampsia or gestational hypertension, treat them as ongoing risk factors, not just past events.
Track your symptoms and numbers over time. If you notice new fatigue, shortness of breath with mild exertion, or unexplained jaw or back pain, don’t ignore it. These can be early signs that your arteries aren’t as healthy as they should be. Early action—getting the right tests and starting interventions—can prevent major problems later.
Now that you know which markers matter, it’s time to put everything together into a practical plan. Here’s how to get started:
1. Request ApoB and Lp(a) tests with your next checkup. Standard cholesterol tests don’t give the full picture, especially for young women. 2. Start omega-3 supplementation. Aim for 2–3 grams daily of combined EPA/DHA, choosing a purified source. 3. If your homocysteine is above 8 umol/L, or you have a known MTHFR variant, add methylfolate (400–800 mcg) and methylcobalamin (500–1,000 mcg) to your daily routine. 4. Build aerobic capacity with zone 2 cardio—150+ minutes per week. Track your progress and adjust as needed.
Stacking these interventions provides coverage across lipid risk, inflammation, and blood vessel health. For women ages 18–39, this protocol is about building resilience now, not just avoiding disease later. The earlier you start, the more benefit you get as you transition through pregnancy, postpartum, and eventually menopause.
As you move forward, remember: your heart health is not determined by any one factor, but by the collective impact of your choices and monitoring.
The decades between 18 and 39 are a critical window for building lifelong cardiovascular health. Estrogen offers some protection, but it is neither complete nor permanent. The risk factors that accumulate now—high ApoB, elevated blood pressure, chronic inflammation—are the same ones that lead to heart attacks and strokes after menopause.
By tracking the right biomarkers, acting on early warning signs, and building a personalized protocol, you can shift your risk curve for decades to come. Every step you take now makes it less likely you will become a heart disease statistic in your 50s and 60s. This is not just about prevention; it’s about building a strong foundation for all the life you want to live.
Empower yourself with knowledge. Use your numbers as feedback, not fear. Take each small action—supplements, exercise, testing—as an investment in your future heart. The earlier you start, the more options you keep open for decades of health and vitality.
The Heart Disease Blind Spot: A Comprehensive Guide to Cardiovascular Health for Women 18–39
Why Your Twenties and Thirties Are the Decades That Decide Your Heart’s Future
Diagram glossary
- 120/80:
- A standard measurement representing normal, healthy human blood pressure.
- 130/85:
- A blood pressure reading indicating elevated levels or stage 1 hypertension.
- B12:
- An essential vitamin crucial for nerve function, red blood cell production, and DNA synthesis.
- CRP:
- C-reactive protein is a blood marker indicating the presence of inflammation in the body.
- estrogen:
- A primary female sex hormone that helps maintain flexible blood vessels and cardiovascular health.
- Homocysteine:
- An amino acid in the blood that can indicate cardiovascular risk at elevated levels.
- LDL:
- Low-density lipoprotein is a cholesterol carrier often associated with increased cardiovascular disease risk.
- Methylfolate:
- The active, bioavailable form of vitamin B9 used to regulate homocysteine levels.
- mmHg:
- Millimeters of mercury is the standard scientific unit used to measure blood pressure.
- MTHFR:
- A gene and enzyme responsible for processing folate and regulating homocysteine levels.
- PCOS:
- Polycystic ovary syndrome is a hormonal disorder that can increase cardiovascular risk in women.
Conclusions
Young women often fall through the cracks when it comes to heart disease risk. By knowing which markers matter—ApoB, Lp(a), hs-CRP, blood pressure, and homocysteine—you can spot problems early, even when you feel perfectly healthy. Omega-3s, B vitamins, and regular aerobic exercise work together to lower risk factors and support your arteries. Early, personalized action in your 20s and 30s is the best way to avoid serious heart problems later. Don’t wait for symptoms—proactive care is your best defense.
This guide is based on current evidence linking early biomarker changes and interventions to future heart risk. Some recommendations—such as specific supplement doses or the benefits of stacking interventions—come from studies in broader or older populations. Individual responses can vary, especially based on genetics, lifestyle, and medical history. Always consult with a healthcare provider before starting new supplements or making major lifestyle changes, especially if you have existing health conditions or are pregnant.
Track this in your stack
See how omega 3 relates to your health goals and monitor changes in your biomarkers over time.
Sources (6)
This article informs how supplementation moves 4 markers.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.
% EPA + DHA in red-blood-cell membranes. Target >= 8% for cognitive protection; most US adults sit at 4-5%.
Amino acid elevated in B-vitamin deficiency. Levels > 11 µmol/L associated with accelerated brain atrophy and cardiovascular event risk.
High-sensitivity C-reactive protein. > 3 mg/L associated with chronic systemic inflammation affecting the brain and vasculature.