
CoQ10 Absorption Is Highly Variable — Your Form, Fat Intake, and Genetics May Determine Whether You're Getting Any Benefit
Why most people are taking a form their body can barely absorb
The surprising truth is CoQ10 often does not absorb well. Many people buy cheap dry capsules. They take them without fat. Then they get little benefit.
This means you should focus on form and timing. Take CoQ10 with a fatty meal. Pick a version that absorbs better. If you want proof, you can test blood CoQ10.
Try ubiquinol 100–200 mg daily with food. If you use ubiquinone, use 200–400 mg daily with fat. Recheck a plasma CoQ10 test after 4–6 weeks. Many people aim for a 2–3× rise from baseline.
- Ubiquinol
- The reduced CoQ10 form; often raises blood CoQ10 more per mg.
- Ubiquinone
- The oxidized CoQ10 form; your body converts it to ubiquinol.
- Ubiquinol:ubiquinone ratio
- A blood marker that may reflect redox balance and conversion between forms.
- Recent
- A branded coq10 formulation used to distinguish one delivery system or manufacturing approach from another in studies and commercial products.
- Oil-based softgel
- CoQ10 dissolved in oil inside a soft capsule; usually absorbs better than dry powder.
- Plasma CoQ10
- A blood test that shows whether your CoQ10 level rose from supplementation.
- Medium-chain triglyceride (MCT) encapsulation
- A formulation technique where CoQ10 is combined with medium-chain fats to improve how well it dissolves and passes through the digestive tract, increasing the amount that enters the bloodstream.
- FSP1
- A cellular enzyme that protects against lipid peroxidation and ferroptosis.
- MCT
- A class of dietary fats with shorter fatty acid chains that are rapidly absorbed.
- oxidoreductase
- An enzyme that catalyzes the transfer of electrons from one molecule to another.
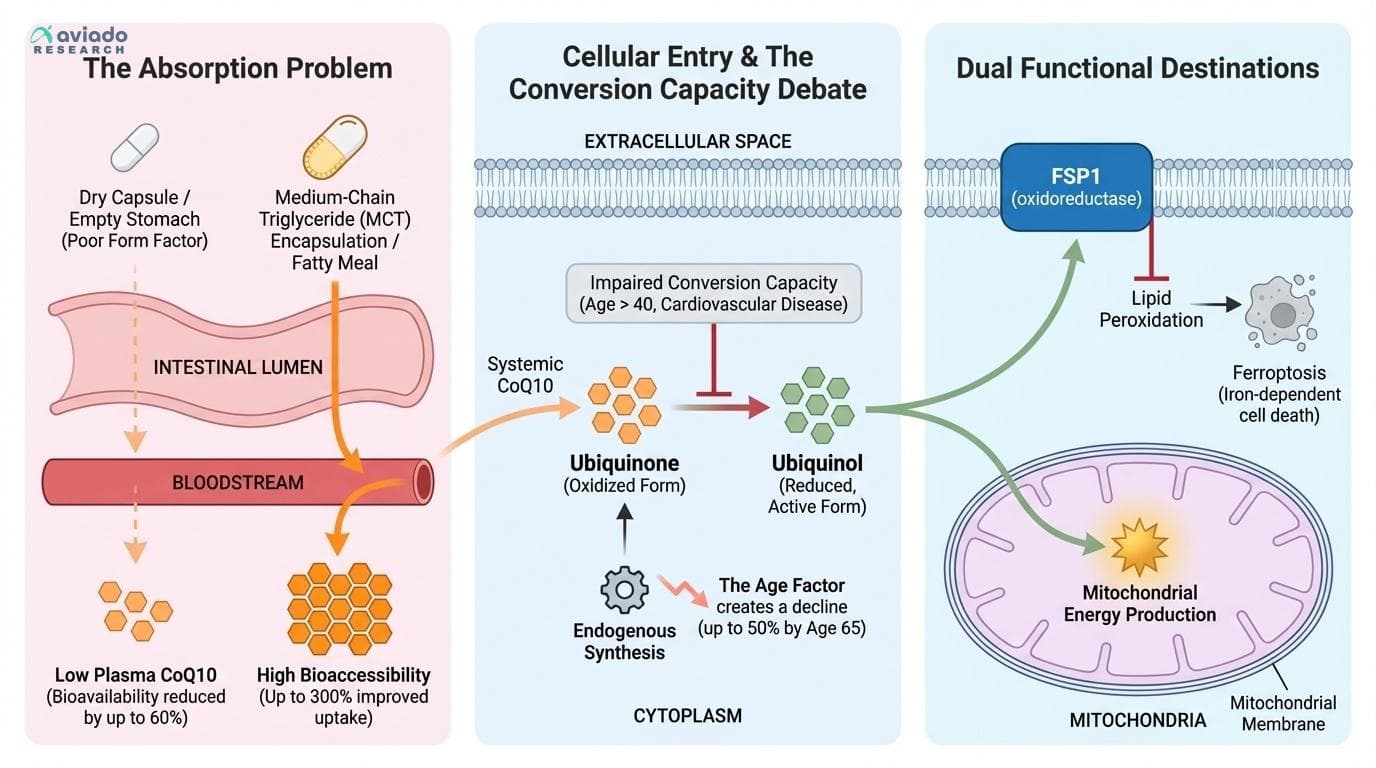
The Absorption Problem Most People Never Consider
The fundamental challenge with CoQ10 supplementation isn't whether it works — it's whether it gets into your system at all. Research consistently shows that CoQ10 absorption varies enormously between individuals, with some people achieving plasma levels 10 times higher than others taking identical doses [1].
This variation stems from several factors that most supplement users never consider. CoQ10 is highly lipophilic, meaning it requires fat for absorption. Taking it on an empty stomach can reduce bioavailability by up to 60% compared to taking it with a fatty meal. Yet many people pop their CoQ10 capsule with morning coffee and wonder why they don't feel more energetic [8].
Even more critical is the form factor. A 2024 study demonstrated that novel medium-chain triglyceride encapsulation can improve CoQ10 bioaccessibility and cellular uptake by up to 300% compared to standard formulations [14]. This suggests that the majority of people taking conventional CoQ10 supplements may be absorbing only a fraction of what they think they're getting.
The age factor compounds this problem. Endogenous CoQ10 synthesis peaks in our twenties and declines steadily thereafter. By age 65, tissue levels can be 50% lower than in young adults. This creates a double burden: older adults need more CoQ10 but absorb supplements less efficiently [8].
Ubiquinone vs. Ubiquinol: The Conversion Capacity Question
The debate between ubiquinone and ubiquinol forms of CoQ10 has evolved beyond simple marketing claims into a question of individual conversion capacity. Ubiquinone is the oxidized form found in most supplements, while ubiquinol is the reduced, active form that provides direct antioxidant protection [6].
Healthy young adults can efficiently convert ubiquinone to ubiquinol in their tissues. However, this conversion capacity declines with age and certain health conditions. Studies show that people with cardiovascular disease often have impaired ubiquinone-to-ubiquinol conversion, potentially explaining why some individuals respond dramatically to CoQ10 supplementation while others see no benefit [6].
Clinical trials comparing the two forms show that both can improve cardiovascular outcomes, but ubiquinol consistently achieves higher plasma levels with lower doses. In one comparative study, 100 mg of ubiquinol produced plasma levels equivalent to 200-300 mg of ubiquinone in older adults [6]. This suggests that for people over 40 or those with existing health concerns, ubiquinol may be the more reliable choice.
The practical implication is that form selection should be personalized rather than universal. If you're young and healthy, ubiquinone at 200-400 mg daily with fat may suffice. If you're older or have cardiovascular concerns, ubiquinol at 100-200 mg daily may be more effective [1].
Beyond Mitochondria: The Ferroptosis Protection Discovery
Recent research has revealed that CoQ10's benefits extend far beyond its well-known role in mitochondrial energy production. The identification of FSP1 as a CoQ10 plasma membrane oxidoreductase has uncovered a completely separate function: protection against ferroptosis, a specific type of cell death driven by iron-dependent lipid damage [15].
Ferroptosis is now recognized as a key mechanism in neurodegeneration, cancer progression, and aging. Unlike other forms of cell death, ferroptosis specifically targets cell membranes through lipid peroxidation. CoQ10, working through the FSP1 system, provides a critical defense against this process by maintaining membrane integrity [15].
This discovery helps explain why CoQ10 shows promise in neurological applications beyond what mitochondrial function alone would predict. The plasma membrane pool of CoQ10 operates independently of mitochondrial CoQ10, suggesting that adequate supplementation needs to support both systems [15].
The ferroptosis protection function also provides a mechanistic basis for CoQ10's role in healthy aging. As endogenous CoQ10 synthesis declines with age, both mitochondrial energy production and membrane protection become compromised. This dual vulnerability may explain why CoQ10 supplementation often produces more noticeable benefits in older adults [4].
Formulation Science: Why Most CoQ10 Supplements Fail
The supplement industry has largely ignored the formulation challenges that make CoQ10 one of the most difficult nutrients to deliver effectively. Standard CoQ10 powder in gelatin capsules has notoriously poor bioavailability, with absorption rates often below 10% [1].
Recent formulation research has identified several breakthrough approaches. Medium-chain triglyceride encapsulation, tested in 2024, showed dramatic improvements in both bioaccessibility and cellular uptake. The MCT matrix appears to enhance CoQ10 solubilization in the digestive tract and facilitate transport across intestinal membranes [14].
Phospholipid complexation represents another promising approach. By binding CoQ10 to phospholipids similar to those in cell membranes, these formulations can improve absorption by 200-400% compared to standard preparations. Some clinical trials have achieved therapeutic plasma levels with doses as low as 60 mg when using advanced delivery systems [1].
Nanoparticle formulations and self-emulsifying drug delivery systems (SEDDS) are also showing promise in research settings. However, these advanced formulations are not yet widely available in consumer supplements. For now, the most accessible high-absorption options are ubiquinol forms and oil-based softgels taken with fatty meals [14].
Testing Your Response: The Plasma CoQ10 Strategy
Given the dramatic individual variation in CoQ10 absorption, testing plasma CoQ10 levels before and after supplementation provides the most reliable way to determine if your regimen is working. Baseline plasma CoQ10 levels vary widely in healthy adults, from 0.4 to 1.9 mg/L, with levels below 0.7 mg/L often considered suboptimal [8].
After 4-6 weeks of consistent supplementation, plasma levels should increase significantly if absorption is adequate. Effective supplementation typically raises plasma CoQ10 to 2-4 mg/L, representing a 2-3 fold increase from baseline. If your levels don't increase substantially, it indicates either poor absorption or inadequate dosing [1].
This testing approach is particularly valuable for people taking medications that may interfere with CoQ10 synthesis or absorption. It's also useful for determining the minimum effective dose, since taking more than necessary provides no additional benefit and increases cost [8].
Some functional medicine practitioners now recommend this test-and-adjust approach as standard practice for CoQ10 supplementation, especially for cardiovascular applications where therapeutic levels are critical for benefit [6].
CoQ10 Absorption Is Highly Variable — Your Form, Fat Intake, and Genetics May Determine Whether You're Getting Any Benefit
Why most people are taking a form their body can barely absorb
Diagram glossary
- FSP1:
- A cellular enzyme that protects against lipid peroxidation and ferroptosis.
- MCT:
- A class of dietary fats with shorter fatty acid chains that are rapidly absorbed.
- oxidoreductase:
- An enzyme that catalyzes the transfer of electrons from one molecule to another.
- triglyceride:
- The main type of fat found in the blood and stored in the body.
Conclusions
CoQ10 works best when you solve the absorption problem first. For many people, that means taking it with fat and choosing an oil-based or MCT-style formula. If you are older or you want a more reliable rise in blood levels, ubiquinol often makes dosing simpler. When you want certainty, plasma CoQ10 before and after is the clearest check that your money is not being wasted.
CoQ10 studies use many different doses, forms, and delivery systems, so results do not always compare cleanly. Blood CoQ10 targets linked to specific outcomes are not firmly set, and higher numbers are not always better. Some high-absorption delivery systems tested in research are not widely available in retail products. Genetic factors that may affect CoQ10 handling are still not well mapped for practical, personalized dosing.
Track this in your stack
See how coq10 relates to your health goals and monitor changes in your biomarkers over time.