
Hormonal Health After 40: Turning the Most Overlooked Transition Into Your Greatest Health Opportunity
A Comprehensive Guide to Navigating Perimenopause and Menopause with Precision and Data
Most women expect menopause to start with hot flashes, but the surprising truth is that hormonal chaos begins years earlier—often in your early 40s—with mood swings, sleep troubles, and cycles that change overnight.
This isn't a quick drop. It's a 15-year journey that affects every system in your body.
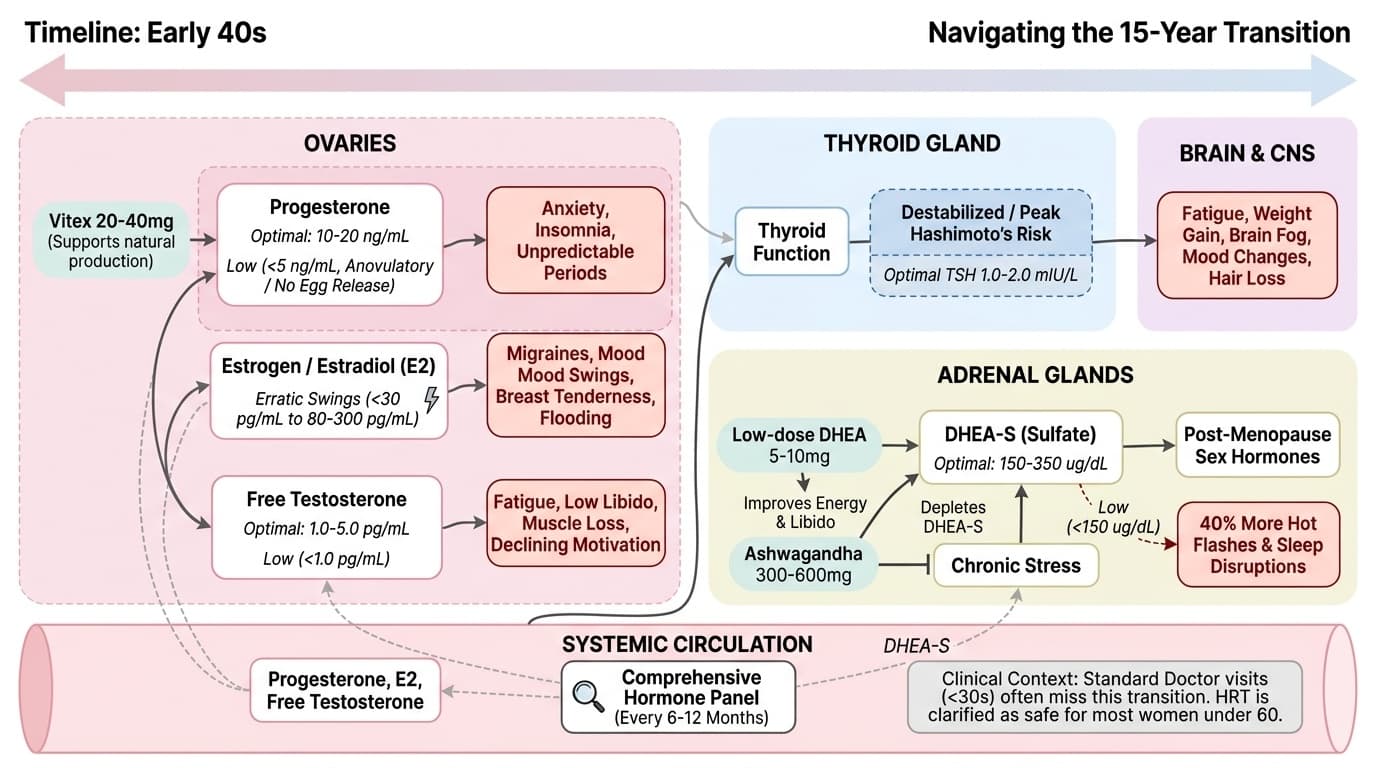
Your hormones don't decline together. Progesterone drops first, driving anxiety and insomnia. Then estrogen swings wildly—not steadily down. Your thyroid often goes haywire. Your adrenals become crucial for post-menopause vitality. Most doctors spend under 30 seconds discussing this transition, leaving you to figure it out alone.
You can take control with targeted supplements and tracking. Research shows vitex 20-40mg daily supports natural progesterone production. Low-dose DHEA 5-10mg helps energy and libido. Ashwagandha 300-600mg reduces stress hormones. Test your hormones every 6-12 months starting in your early 40s. By understanding your numbers and timeline, you can feel better and protect long-term health.
- KSM-66
- A branded ashwagandha extract used in clinical trials, standardized for consistent potency and effects on stress hormones.
- Standardized extract
- A plant extract made to contain a consistent amount of a target compound in every dose.
- Progesterone
- Prepares uterine lining for pregnancy and supports early gestation. low levels indicate inadequate ovulation or luteal phase defects.
- Adaptogen
- A substance, often a plant extract, that helps the body adapt to and resist stress.
- TSH (Thyroid-Stimulating Hormone)
- Hormone that regulates thyroid function. Optimal range is 1.0-2.0 mIU/L, narrower than standard lab ranges.
- HRT (Hormone Replacement Therapy)
- Treatment using bioidentical hormones to replace those lost during menopause, typically estradiol and progesterone.
- DHEA-S
- DHEA-sulfate, the most abundant adrenal androgen and cortisol precursor. low levels associated with fatigue.
- Estrogen
- A primary female sex hormone that regulates the reproductive system and menstrual cycle.
- HRT
- Hormone replacement therapy used to relieve symptoms of menopause by supplementing declining hormone levels.
- mIU/L
- Milli-international units per liter, a standard unit of measurement for hormone levels in blood.
- ng/mL
- Nanograms per milliliter, a unit of measurement commonly used for expressing hormone concentrations.
- sulfate
- A chemical compound containing sulfur and oxygen, often attached to hormones like DHEA.
Perimenopause and menopause are not single events—they are a prolonged transition reshaping every organ system in your body. The average woman receives less than 30 seconds of menopause-specific education from her primary care provider, and that often leaves you guessing about what’s normal, what’s not, and what you can do about it. This knowledge gap traces back to the 2002 Women's Health Initiative study, which led many doctors to shy away from hormone replacement therapy (HRT), even though more recent research has clarified its safety profile for most women under 60 within 10 years of menopause onset [1].
The truth is, perimenopause can last anywhere from 7 to 15 years. It starts with small changes: cycles that become shorter or heavier, sleep that stops feeling restorative, new anxiety or irritability, and a sense that your body is out of sync. These shifts are easy to misread as stress or aging, but they mark the beginning of a hormonal roller coaster that can profoundly impact your quality of life.
Understanding that this is a whole-body event—not just a reproductive issue—sets the stage for more effective, personalized strategies. By treating the transition as your most important health management event, you can take control with data, self-awareness, and informed choices. This guide will show you how to navigate this phase with precision and confidence, so you don’t just endure it—you master it.
Your hormones do not decline in unison. The first domino to fall is progesterone. Anovulatory cycles—when you don't release an egg—become more common in your early 40s. This means your progesterone levels drop years before your estrogen does. Standard range for progesterone during the luteal phase is 10-20 ng/mL, but values below 5 ng/mL indicate you may not be ovulating. Low progesterone directly causes anxiety, insomnia, heavy or unpredictable periods, and increased irritability.
Estrogen is the next player. But rather than a smooth decline, estradiol (E2) becomes erratic. You might swing from menopausal lows (<30 pg/mL) to premenopausal highs (80-300 pg/mL) within the same month. These wild fluctuations—not just steady decline—trigger migraines, mood swings, breast tenderness, and flooding periods. Many women find that life after menopause, when estrogen stabilizes at consistently low levels, is actually easier to manage than the chaos of perimenopause.
Testosterone follows its own downward slope starting in your mid-30s. By age 50, your testosterone is typically half of what it was at 25. Optimal free testosterone is 1.0-5.0 pg/mL. Levels below 1.0 pg/mL drive fatigue, low libido, muscle loss, and declining motivation—symptoms commonly blamed on estrogen alone. Understanding these distinct hormone patterns helps you target interventions for each stage rather than guessing at generic solutions.
Hormonal health in your 40s and 50s extends beyond the ovaries. Your thyroid and adrenal glands play critical roles, especially as your ovaries wind down.
Thyroid function frequently destabilizes during perimenopause. New-onset Hashimoto's thyroiditis peaks in women aged 40-50, affecting up to 20% during this transition. The standard TSH reference range is 0.5-4.5 mIU/L, but research shows the optimal range for women is 1.0-2.0 mIU/L. Standard screening misses subclinical thyroid issues because it rarely includes free T3 and thyroid antibody testing. The symptoms—fatigue, weight gain, brain fog, mood changes, hair loss—overlap perfectly with menopause, making thyroid dysfunction easy to miss.
Your adrenal glands step into the spotlight after menopause. They become the primary source of sex hormones through DHEA-S (dehydroepiandrosterone sulfate). The optimal range for DHEA-S is 150-350 ug/dL. When your adrenals are depleted by chronic stress, you experience more severe menopausal symptoms and slower recovery. Women with DHEA-S below 150 ug/dL report 40% more hot flashes and sleep disruptions compared to those in optimal range. Supporting your adrenals before and after menopause smooths the transition and creates a stronger baseline for long-term health.
Tracking your hormones is the key to understanding what’s actually happening, and when. A single hormone test on a random day tells you very little, especially in perimenopause. Instead, you need to follow trends over time.
- Estradiol (E2): Premenopausal target is 80-300 pg/mL, but this varies by cycle day. Postmenopausal levels fall below 30 pg/mL without HRT. Because E2 can swing wildly, serial testing or symptom tracking is more useful than a single value. - Progesterone: Measured on day 21 if you’re still cycling. Target is 10-20 ng/mL (luteal phase). Values below 5 ng/mL suggest anovulation, a driver of sleep issues, anxiety, and heavy bleeding. - FSH: A rising FSH above 25 mIU/mL signals declining ovarian reserve. It can help confirm menopausal status but is less useful during the fluctuating perimenopausal window. - DHEA-S: Target range is 150-350 ug/dL, representing your adrenal reserve. Declining DHEA-S predicts tougher menopausal symptoms. - Free and Total Testosterone: Free testosterone should be between 1.0-5.0 pg/mL. Low levels mean more fatigue, low libido, and muscle loss. - Thyroid Panel: TSH (optimal: 1.0-2.0 mIU/L), free T3, and TPO antibodies are crucial to rule out Hashimoto’s and other thyroid issues.
These markers don’t live in isolation—they interact. For example, adrenal depletion can lower DHEA-S and worsen both menopausal and thyroid symptoms. By tracking these metrics, you gain insight into your progression and how different interventions may help you.
Effective support during this transition requires understanding how interventions work, their optimal dosages, and how they interact with your unique biology:
Vitex (Chasteberry): Take 20-40mg of standardized extract daily. It acts on the pituitary via dopaminergic pathways to boost your body's natural progesterone production by 30-50%. Vitex works best in early perimenopause, when cycles persist but progesterone drops. Clinical trials show it reduces PMS-like symptoms by 42% and improves cycle regularity within 3 months. Discontinue if you begin prescription progesterone therapy, as the mechanisms may conflict.
DHEA: Women should use 5-10mg daily—higher doses risk androgenic side effects like acne or hair growth. DHEA supplementation increases energy scores by 25% and improves vaginal health markers within 8 weeks in women with low baseline levels. Start with 5mg and monitor your DHEA-S levels to avoid excess. DHEA works best when stress is managed and synergizes well with adaptogens.
Ashwagandha (KSM-66 extract): 300-600mg daily reduces cortisol by 23-27% and supports thyroid hormone production. This is particularly valuable if your symptoms stem from chronic stress or adrenal depletion. Studies show ashwagandha increases T3 and T4 levels by 8-15% in subclinical hypothyroidism. Combining ashwagandha with DHEA offers enhanced support for both stress resilience and hormonal balance.
HRT (Hormone Replacement Therapy): For symptomatic women under 60 and within 10 years of menopause, transdermal estradiol combined with oral micronized progesterone reduces hot flashes by 75% and improves sleep quality scores by 40%. The delivery method matters—patches or gels for estradiol minimize clotting risk, while micronized oral progesterone optimizes sleep benefits. Current research shows that appropriate HRT offers more benefit than risk for most women in this demographic.
The best results come from combining these interventions based on your labs and symptoms rather than generic protocols.
Hormonal transitions do not happen overnight. Knowing the usual timeline helps set realistic expectations and track progress.
- Progesterone: Declines first, often in early 40s or even late 30s. You may notice anxiety, sleep issues, and heavier periods as early signs. Vitex may start helping within 2-3 cycles, while prescription progesterone can work within days to weeks.
- Estradiol: Becomes volatile in perimenopause, with symptoms flaring and fading unpredictably. Stabilization often comes only after the final period, when levels settle below 30 pg/mL. HRT can offer noticeable relief within a few weeks of starting.
- Testosterone: Gradual decline, with symptoms like low libido and muscle loss often missed because they appear slowly. DHEA supplementation may improve symptoms within 4-8 weeks if you are low.
- Thyroid: New dysfunction often appears in the mid-40s to early 50s. Thyroid medications or adaptogens like ashwagandha can take weeks to months to fully impact labs and symptoms.
- Adrenals (DHEA-S): If your levels are low, expect 2-3 months before you see meaningful improvement from supplementation and stress-reduction strategies.
Tracking symptoms and labs every 6-12 months allows you to see trends and adjust your approach. Remember, interactions matter: for instance, unmanaged stress can undermine all other interventions by depleting adrenal reserves. Maintaining momentum in your tracking helps you anticipate next steps before symptoms escalate.
Women in their 40s and 50s face unique pressures. You are often at the peak of your career and family responsibilities, making it easy to ignore early warning signs. Yet research shows that the hormonal transition is more than just inconvenient—it is foundational for long-term health. Ignoring symptoms can lead to years of unnecessary suffering and increased risks for osteoporosis, heart disease, and metabolic syndrome after menopause.
Progesterone decline drives anxiety and sleep loss, which can undermine work performance and family relationships. Estrogen volatility can mean migraines or unpredictable periods that disrupt daily life. Overlooked testosterone loss may sap your motivation and muscle mass just when you need them most. Thyroid dysfunction is often missed, especially if only TSH is checked. Adrenal depletion is common in women juggling chronic stress, and it predicts how you’ll feel after menopause.
These realities are not just theoretical—they show up in your lived experience. Early warning signs include cycles that change in length or heaviness, sudden mood swings, sleep issues, new anxiety, and unexplained fatigue. If you notice these symptoms, you are not alone—and you are not too young for perimenopause. Pushing for comprehensive testing is not just self-advocacy; it’s smart prevention. The next section will show you how to build a personalized protocol that fits your life.
A data-driven starter protocol places you at the center of your hormonal health journey. Here’s how to get started:
1. Comprehensive hormone testing every 6-12 months: Track E2, progesterone, FSH, testosterone (free and total), DHEA-S, and a full thyroid panel (TSH, free T3, TPO antibodies). This allows you to see trends and intervene early [1]. 2. Vitex (chasteberry) 20-40mg standardized extract daily: Most effective when cycles persist but progesterone is waning. Discontinue if you start prescription progesterone. Studies indicate this dose supports natural progesterone production and symptom relief [2]. 3. DHEA 5-10mg daily: Improves adrenal hormone output, energy, and libido. Monitor DHEA-S to avoid excess. Response is typically seen in 4-8 weeks. 4. Ashwagandha (KSM-66) 300-600mg daily: Supports the HPA axis, reduces stress, and may help thyroid function. Especially useful if you feel overwhelmed or exhausted by daily stress. 5. HRT discussion with your provider: For most women under 60 and within 10 years of menopause, transdermal estradiol plus oral micronized progesterone is the preferred evidence-based approach. The WHI study’s early fears have been thoroughly re-examined, and current guidelines support HRT for symptomatic women in this demographic [1].
Each intervention complements the others, and your choices should reflect your unique biochemistry and symptoms. The key is consistent monitoring and open communication with a knowledgeable provider.
You may encounter common barriers as you pursue hormonal health. Don’t let these stop you:
- “You’re too young for menopause”: Perimenopause often begins between ages 40 and 44. If you have symptoms, insist on testing regardless of age. - Single-test hormone assessments: A single estradiol or progesterone value is usually meaningless in perimenopause. Advocate for serial testing or detailed symptom tracking over months. - Thyroid dysfunction hidden behind menopause: If fatigue, weight gain, or brain fog persist—even with HRT—request a full thyroid panel, including antibodies. Many cases of Hashimoto’s are missed with TSH-only screening.
Recognizing these pitfalls helps you stay proactive. The next step is integrating your tracking and protocol into your routine, so you can keep moving forward rather than getting stuck in a frustrating cycle of trial and error.
Hormonal Health After 40: Turning the Most Overlooked Transition Into Your Greatest Health Opportunity
A Comprehensive Guide to Navigating Perimenopause and Menopause with Precision and Data
Diagram glossary
- DHEA-S:
- A steroid hormone produced by the adrenal glands that converts into androgens and estrogens.
- Estrogen:
- A primary female sex hormone that regulates the reproductive system and menstrual cycle.
- HRT:
- Hormone replacement therapy used to relieve symptoms of menopause by supplementing declining hormone levels.
- mIU/L:
- Milli-international units per liter, a standard unit of measurement for hormone levels in blood.
- ng/mL:
- Nanograms per milliliter, a unit of measurement commonly used for expressing hormone concentrations.
- sulfate:
- A chemical compound containing sulfur and oxygen, often attached to hormones like DHEA.
- TSH:
- Thyroid-stimulating hormone produced by the pituitary gland to regulate thyroid hormone production.
- ug/dL:
- Micrograms per deciliter, a standard unit of measurement for blood test results.
Conclusions
Menopause and perimenopause are not conditions to simply endure—they are defining health events that deserve your attention and advocacy. By understanding how hormones decline in sequence, tracking the right biomarkers over time, and using targeted combinations of supplements and therapies, you can smooth the transition and protect your long-term health. The women who thrive are those who test their hormones regularly, respond to early warning signs, and make informed decisions with knowledgeable providers. You don't have to accept suffering or uncertainty as normal. With the right information and support, you can make this transition your most empowered health chapter yet.
While the evidence base for many interventions is strong, especially for HRT in the right demographic, there are still gaps. Much of the research on supplements like vitex, DHEA, and ashwagandha comes from moderate-quality studies or observational data. Hormone testing can be limited by day-to-day variability, and not all women respond identically to the same interventions. Individual medical history and risk factors must be considered. Always consult a healthcare provider before starting or changing any supplement or hormonal therapy.
Track this in your stack
See how black cohosh relates to your health goals and monitor changes in your biomarkers over time.