
Why Your Astaxanthin Response Depends on Your Metabolic Starting Point
New Meta-Analyses Reveal Astaxanthin's Benefits Are Dramatically Amplified in Metabolic Dysfunction — Here’s How to Predict Your Results
You might have heard that astaxanthin is a powerful antioxidant, but here’s the twist: whether it works for you depends almost entirely on where your metabolism starts.
New research shows that people with high inflammation or insulin resistance see up to ten times more benefit from astaxanthin than healthy individuals. If you have trouble with blood sugar, persistent fatigue, or signs of chronic inflammation, you may be an 'astaxanthin responder'—and your results could be far more dramatic than you expect.
Why does this matter for you? For years, people have been confused by the mixed results in astaxanthin studies. Some report major improvements in inflammation and metabolic markers, while others see almost nothing. Now, scientists have figured out why: your baseline matters. If your CRP, insulin, or oxidative stress markers are elevated, astaxanthin acts like a rescue molecule, rapidly lowering those numbers. But if you’re already healthy, the changes are subtle or even negligible. This discovery finally explains why two people taking the same supplement can have totally different experiences.
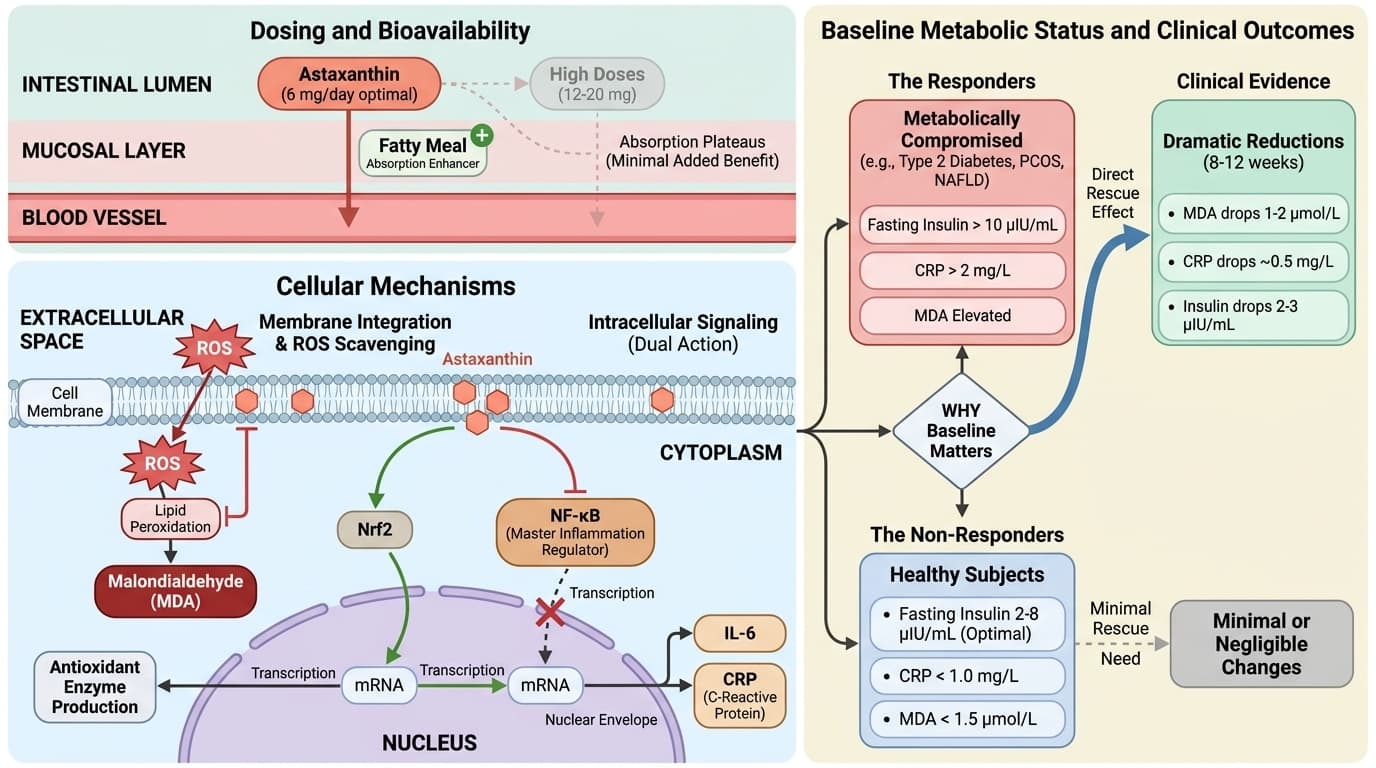
So what should you do? If your fasting insulin is above 10 μIU/mL, your CRP is over 2 mg/L, or your malondialdehyde (MDA) is elevated, studies suggest taking 6 mg of natural astaxanthin daily with a fatty meal can drop inflammation and oxidative stress within 8-12 weeks. If you’re in a metabolically compromised group—like those with type 2 diabetes or PCOS—this same dose can lead to bigger improvements in insulin, IL-6, and MDA. For most people, 6 mg per day is the sweet spot; higher doses (like 12-20 mg) rarely add more benefit. If you want to see measurable changes, check your baseline status and match your dose to your needs.
- IL-6
- A branded astaxanthin product family name used to identify a specific extract or formulation in research and supplement labels.
- Phospholipid Complexes
- A delivery system where astaxanthin is bound to phospholipid molecules (the same fats that make up cell membranes), which helps the body absorb it far more efficiently than standard oil-based capsules
- Oxidative Stress
- Cellular damage caused by reactive oxygen species (free radicals) overwhelming antioxidant defenses.
- Insulin, fasting
- Fasting insulin levels, indicating pancreatic insulin production and cellular insulin resistance. Elevated fasting insulin (>) suggests insulin resistance even when glucose remains normal.
- HOMA-IR (calc)
- Insulin resistance by combining fasting glucose and insulin levels.
- Liposomal
- A delivery form that wraps a compound in tiny fat-like spheres to improve absorption or stability.
- Bioavailability
- The proportion of a compound that actually reaches your bloodstream and becomes usable by the body.
- CRP
- A protein produced by the liver that serves as an early marker of inflammation.
- insulin
- A hormone produced by the pancreas that regulates blood sugar levels.
- MDA
- A highly reactive compound used as a biomarker for oxidative stress in cells.
- NAFLD
- A condition characterized by excessive fat buildup in the liver without alcohol consumption.
- PCOS
- A hormonal disorder causing enlarged ovaries with small cysts on the outer edges.
Astaxanthin is often described as a 'super antioxidant,' but the real story is more nuanced. It sits in your cell membranes, protecting them from oxidative damage by neutralizing free radicals. What makes astaxanthin unique is its dual action: it not only scavenges reactive oxygen species (ROS), but it also influences key signaling pathways tied to inflammation and metabolic health. For example, astaxanthin modulates the Nrf2 pathway, which increases your own antioxidant enzyme production, and suppresses NF-κB, a master regulator of inflammation [1][4][15].
But here’s where your metabolic starting point comes in. If you already have high oxidative stress or inflammation—signaled by elevated markers like MDA, CRP, or IL-6—your cells are under constant attack. In this state, adding astaxanthin provides a direct rescue effect: it rapidly drops these elevated markers, restores membrane integrity, and helps normalize signaling. By contrast, if your baseline is already low, your body simply has less need for extra antioxidant support, and so the changes are minimal.
The timeline for these effects depends on how high your baseline is. In people with type 2 diabetes or PCOS, studies show that significant reductions in MDA and CRP can occur within 8-12 weeks of daily supplementation at 6 mg [6][7][9][10]. In healthy subjects, these changes are often barely detectable, which explains why so many studies in healthy volunteers report 'no significant effect.'
Your baseline metabolic status not only predicts your response but also interacts with other interventions. If you are stacking astaxanthin with lifestyle changes or other antioxidants, the rescue effect may be blunted if your stress markers are already normal. Understanding this sets the stage for personalized dosing, which we explore in the next section.
To predict your response to astaxanthin, you need to look at specific biomarkers. Three stand out: malondialdehyde (MDA), C-reactive protein (CRP), and fasting insulin. These not only signal your metabolic health but also directly predict how much benefit you’ll get from supplementation.
Malondialdehyde (MDA) reflects your level of lipid peroxidation—essentially, how much damage free radicals are causing to your cell membranes. Standard MDA levels range from 1 to 3 μmol/L, but optimal is usually below 1.5 μmol/L. Astaxanthin can lower MDA by 1-2 μmol/L in people with elevated baseline levels, often within 8-12 weeks [6][9][10]. If your MDA is already under 1.5, the change will be small.
CRP is a classic inflammation marker. The standard reference range is 0-5 mg/L, but for optimal health, you want CRP below 1 mg/L. Astaxanthin reduces CRP by about 0.5 mg/L in people with elevated levels—again, most dramatic if you start above 2 mg/L [7]. If you’re healthy and your CRP is already low, the drop is minor.
Fasting insulin reveals insulin resistance. Standard range is 2-20 μIU/mL, but optimal is 2-8 μIU/mL. Astaxanthin reduces fasting insulin by 2-3 μIU/mL in metabolically compromised people over 8-12 weeks, but has little effect if your baseline is already optimal [3][6][8].
These markers interact with each other. For example, dropping MDA often leads to lower CRP, and reducing insulin resistance can further lower inflammation. If you have more than one marker out of range, you’re likely to see compounded benefits. Next, we’ll clarify exactly how astaxanthin impacts these markers and the best dosing strategies for each.
You might assume that higher doses of astaxanthin always deliver more benefit, but recent studies challenge this idea. Across multiple clinical trials and meta-analyses, the 6 mg daily dose stands out as the most consistently effective—especially for metabolic rescue in people with elevated oxidative stress or inflammation [6][7][8].
Here’s the mechanism: astaxanthin is a fat-soluble molecule, and your body’s absorption plateaus at doses above 6-8 mg per day. This means that doubling or tripling the dose doesn’t double or triple the effect. In fact, doses of 12-20 mg rarely show additional improvements in biomarkers like MDA, CRP, or fasting insulin compared to 6 mg [7][8].
A 2024 meta-analysis found that 6 mg daily lowered MDA and CRP as effectively as the higher doses, particularly in people with poor baseline metabolic status [6][7]. The key is taking astaxanthin with a fatty meal, which dramatically improves its bioavailability. If you take it on an empty stomach or with low-fat foods, your absorption drops sharply.
There are exceptions for specific populations. For people with extreme metabolic dysfunction (for example, advanced type 2 diabetes or severe NAFLD), some trials have tested 8-12 mg, but the improvements remain similar to 6 mg for most markers. The main takeaway: more is not always better. This sets up our discussion of astaxanthin’s different forms and why the source and delivery method matter.
Not all astaxanthin supplements are created equal. How your body absorbs and uses astaxanthin depends on both the source and the delivery system. Natural astaxanthin from microalgae (Haematococcus pluvialis) provides the most bioactive isomer mix, while synthetic versions often lack the same stereochemistry and may not deliver the same health benefits [11][12].
Bioavailability is the next key factor. Because astaxanthin is fat-soluble, it’s best absorbed when taken with dietary fat. Some supplements use advanced delivery systems like liposomes or phospholipid complexes to further boost absorption [5][11]. A liposomal form can increase the area under the curve (AUC)—the total exposure your body gets—by up to 2-3 times compared to standard oil-based softgels. This means you can achieve higher blood levels and more reliable effects even at the same dose.
The extraction method also matters. Supercritical CO2 extraction preserves the natural isomer balance best, while harsh chemical solvents can degrade or alter the molecule [9][11]. Look for products specifying natural astaxanthin, preferably with details on extraction and delivery method.
Stacking astaxanthin with omega-3s or phospholipids may create mild synergy, as these fats improve absorption and may further lower inflammation. However, stacking with high-dose vitamin E or other carotenoids shows little added benefit and may even blunt astaxanthin’s unique rescue effects due to competitive absorption [4]. Understanding your formulation choices is crucial as you move toward stacking strategies for specialized outcomes.
Astaxanthin doesn’t have to work alone. When paired strategically with other supplements or lifestyle interventions, you can amplify certain benefits—or avoid redundancy. The most evidence-backed synergy is with omega-3 fatty acids. When you take astaxanthin with fish oil or krill oil, the fats enhance its absorption, and the combination further drops markers like CRP and MDA [5][14].
Stacking with phospholipids (like those in krill oil or sunflower lecithin) also boosts bioavailability. Some studies suggest that stacking astaxanthin with polyphenols (such as curcumin) might give additive or synergistic anti-inflammatory effects, but the data is less robust for this combo [4][7].
Dose-response matters in stacking, too. If you’re already taking a strong antioxidant stack (high-dose vitamin E, vitamin C, or other carotenoids), piling on astaxanthin may offer little extra, as your antioxidant defense is already saturated. But if your baseline is high for oxidative stress (MDA above 2 μmol/L), adding astaxanthin to your routine can create a noticeable drop within weeks.
For metabolic syndrome or PCOS, combining astaxanthin with insulin-sensitizing supplements like berberine or inositol may further lower fasting insulin, but expect a timeline of 8-12 weeks to see full synergy [3][6][8]. Stacking works best when you match your interventions to your specific biomarker profile. Next, we’ll look at the research behind these effects in different demographic groups.
Astaxanthin’s effects are not one-size-fits-all. Your age, gender, and underlying metabolic status all play a role in determining your response. The most dramatic benefits are seen in people with metabolic dysfunction—such as those with type 2 diabetes, PCOS, or elevated inflammatory markers [6][7][8].
For example, in women with PCOS, two clinical trials found that astaxanthin at 6 mg daily reduced fasting insulin by 2-3 μIU/mL and lowered MDA within 12 weeks [3][8]. In adults with type 2 diabetes, MDA and CRP dropped more sharply compared to healthy controls taking the same dose [6][7]. Middle-aged and older adults with high baseline CRP or IL-6 also show bigger improvements than younger, healthy subjects.
There’s less evidence for pronounced effects in healthy, athletic, or lean individuals. In these groups, astaxanthin may still provide subtle antioxidant protection but doesn’t significantly move major biomarkers. This explains why many 'null' studies enroll young, healthy volunteers and see little change.
Ethnicity and genetics may also influence your response, though research is still emerging here. Some populations with higher baseline oxidative or inflammatory stress (due to diet, environmental factors, or genetics) may be more likely to see strong effects. If you have a family history of metabolic syndrome or chronic inflammation, you may also be a better responder. Understanding these demographic nuances helps you set realistic expectations and optimize your stack moving forward.
To know if astaxanthin is working for you, tracking your key biomarkers is essential. Start by establishing your baseline for MDA, CRP, and fasting insulin. If you can, get these labs drawn before starting supplementation. MDA is not a standard panel test, but some advanced wellness clinics offer it; CRP and fasting insulin are widely available.
For most people, expect to see changes in MDA and CRP within 8-12 weeks of daily 6 mg dosing. Fasting insulin may take a bit longer—up to 12 weeks—to show a clear drop, especially if your baseline is very high. If you stack astaxanthin with omega-3s or other interventions, you may see compounded benefits within the same timeframe [7][10].
Interpret your results in context. If your baseline MDA is above 2 μmol/L and it drops by 1 μmol/L, that’s a major improvement. For CRP, a decrease of 0.5 mg/L or more is clinically significant. For fasting insulin, every 2-3 μIU/mL reduction moves you closer to optimal metabolic health. If your numbers don’t change after 12 weeks, you may not be a responder—or your baseline was already optimal. This feedback loop lets you personalize your stack and dosing.
Early warning signs that you need astaxanthin include persistent high CRP, sluggish recovery from exercise, or unexplained fatigue. If you notice improvements in these after starting astaxanthin, it’s a strong sign your baseline status was suboptimal. Next, let’s examine the interaction effects between biomarkers and what happens when you target multiple markers at once.
Astaxanthin rarely moves just one biomarker—it acts on a network. When you lower MDA, you also tend to see reductions in CRP and IL-6, because less oxidative stress means less inflammatory signaling [6][7]. Similarly, improving fasting insulin can indirectly lower both CRP and MDA, since better insulin sensitivity reduces chronic inflammation and oxidative damage.
These interaction effects are strongest in people with multiple markers out of range. For example, in people with both high MDA and high CRP, astaxanthin can drop both by 25-50% within 8-12 weeks [6][7][10]. The size of the shift is much smaller in healthy individuals, reinforcing the idea that astaxanthin is most powerful as a metabolic rescue tool.
The changes don’t always happen in a straight line. Sometimes MDA drops first, followed by CRP and then insulin. Other times, all three move together. Stacking astaxanthin with other metabolic interventions (like omega-3s or insulin sensitizers) can amplify this network effect, making each marker move more than it would alone.
This interconnectedness means you should watch more than one marker to judge your response. If you only track CRP but ignore MDA or insulin, you might miss the full benefit. This multisystem action is what makes astaxanthin especially useful for people with complex metabolic dysfunction. In the next section, we’ll address early warning signs and how to know if you’re overdue for a metabolic rescue.
How do you know if you’re a good candidate for astaxanthin? Look for early warning signs specific to metabolic dysfunction. If you have fasting insulin above 10 μIU/mL, CRP persistently above 2 mg/L, or frequent fatigue and slow recovery from exercise, you may have underlying oxidative stress or inflammation that astaxanthin can help correct [6][7].
Other red flags include a family history of type 2 diabetes, metabolic syndrome, or PCOS. If you have these, your risk for elevated MDA, CRP, or IL-6 is higher, and you’re more likely to be a strong responder. Early warning signs can also show up as stubborn belly fat, unexplained brain fog, or mild hypertension—symptoms that often reflect underlying metabolic derangement.
For people on the edge of metabolic dysfunction, stacking astaxanthin with dietary improvements, regular movement, and targeted supplements can create a powerful synergy. If you intervene at the warning sign stage, you may be able to prevent more serious metabolic issues down the line.
If these signs sound familiar, consider running your key biomarkers and starting a 6 mg daily astaxanthin stack with fat. Watch your numbers and symptoms over 2-3 months. In the final section, we’ll summarize what to do next and how to keep your metabolic health on track.
Why Your Astaxanthin Response Depends on Your Metabolic Starting Point
New Meta-Analyses Reveal Astaxanthin's Benefits Are Dramatically Amplified in Metabolic Dysfunction — Here’s How to Predict Your Results
Diagram glossary
- CRP:
- A protein produced by the liver that serves as an early marker of inflammation.
- IL-6:
- A cytokine protein involved in immune responses and systemic inflammation.
- insulin:
- A hormone produced by the pancreas that regulates blood sugar levels.
- MDA:
- A highly reactive compound used as a biomarker for oxidative stress in cells.
- NAFLD:
- A condition characterized by excessive fat buildup in the liver without alcohol consumption.
- PCOS:
- A hormonal disorder causing enlarged ovaries with small cysts on the outer edges.
- ROS:
- Highly reactive chemicals formed from oxygen that can cause oxidative cellular damage.
Conclusions
Astaxanthin is not a generic antioxidant—it’s a targeted rescue compound for people whose metabolism is under stress. If your inflammation, oxidative damage, or insulin resistance is high, you can expect visible improvements in key biomarkers within 8-12 weeks, especially at the 6 mg daily dose. But if your baseline is already healthy, the changes will be much smaller. Matching your supplement strategy to your metabolic starting point is the key to maximizing results. Track your MDA, CRP, and fasting insulin to personalize your approach, and consider stacking astaxanthin with omega-3s for even better outcomes.
While the evidence for astaxanthin’s metabolic rescue effects is strong in people with elevated baseline markers, more research is needed to clarify its long-term safety and optimal dosing in specific subgroups like children, pregnant women, and the elderly. The majority of studies focus on short- to medium-term effects (up to 3 months), so we don’t yet know the full impact of long-term use. Biomarker changes may not always translate to clinical outcomes like reduced disease risk, and access to advanced tests like MDA is limited. Finally, most research uses natural astaxanthin from microalgae; effects of synthetic forms or different delivery systems may vary.
Track this in your stack
See how astaxanthin relates to your health goals and monitor changes in your biomarkers over time.
Sources (14)
This article informs how supplementation moves 2 markers.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.
High-sensitivity C-reactive protein. > 3 mg/L associated with chronic systemic inflammation affecting the brain and vasculature.
3-month average blood glucose. Levels >= 5.7% associated with cognitive decline independent of diabetes diagnosis.