
Why Your Collagen Supplement Probably Isn't Working (And How to Tell)
The New Science of Mechanobiology and Collagen Response
You might be surprised to learn that swallowing collagen supplements does almost nothing for your skin, joints, or bones—unless your body is already primed for collagen synthesis by physical stress.
Despite the billions spent every year on collagen powders and gummies, most people see little or no benefit because they are missing the real trigger for collagen production: mechanical loading. If you’re relying on supplements alone, you’re likely leaving results on the table.
The latest research reveals that collagen isn’t just a structural protein; it’s a highly responsive system that adapts to force and motion. Your body’s collagen fibers only become stronger, thicker, or more organized when they’re challenged by tension, pressure, or stretching—like you get from weightlifting, resistance bands, or even brisk walking. Supplements can provide the raw materials, but without the right mechanical signals, those ingredients simply don’t get used for new collagen assembly.
If you want real results—firmer skin, stronger tendons, or healthier joints—pair 10-15 grams of hydrolyzed collagen daily with targeted resistance training at least three times a week. For skin benefits, combine with 50 mg of vitamin C and 100 mg of hyaluronic acid, taken 30 minutes before your workout. That’s the protocol that recent studies show is most likely to increase measurable markers of collagen synthesis and visible tissue firmness. The takeaway: Don’t just take collagen—make your body use it.
- CTX-1
- A branded collagen product family name used to identify a specific extract or formulation in research and supplement labels.
- Liposomal
- A delivery form that wraps a compound in tiny fat-like spheres to improve absorption or stability.
- Bioavailability
- The proportion of a compound that actually reaches your bloodstream and becomes usable by the body.
- Hydrolyzed collagen
- A form of collagen that has been broken down into smaller peptides for easier absorption. Important because it is the main type used in supplements.
- Procollagen type I N-terminal propeptide (PINP)
- A blood marker of new collagen formation. Tracking PINP helps you see if your interventions are working.
- Matrix metalloproteinases (MMPs)
- A family of enzymes that break down collagen. Levels rise with inflammation or inactivity, leading to tissue breakdown.
- Growth Differentiation Factor 15 (GDF-15)
- Top aging biomarker per meta-analysis. Stress-responsive cytokine elevated in aging, cancer, heart failure, and chronic disease.
- bovine
- Relating to cattle, often used to describe a primary source of dietary collagen supplements.
- Collagen
- The primary structural protein forming the backbone of skin, bones, tendons, and ligaments.
- hydroxyproline
- An amino acid unique to collagen that stabilizes its triple-helix structure.
- III
- A specific type of structural collagen commonly found alongside type I in connective tissues.
- marine
- Relating to the sea, commonly referring to collagen sourced from fish or aquatic life.
Collagen is the most abundant protein in your body, forming the backbone of skin, bones, tendons, and ligaments. More than 28 types of collagen exist, but types I, II, and III make up the vast majority of your connective tissues [1,4]. Type I collagen alone accounts for about 90% of the collagen in your body and is particularly important for bone strength and skin elasticity [2].
Each collagen molecule is a triple helix made from three protein chains, which then assemble into larger fibrils and fibers. This unique structure gives collagen its strength and flexibility. Fibrillar collagens, especially types I and III, create a scaffold that supports tissues under tension—think of them as the rebar in your biological concrete [4]. Collagen's interactions with water and minerals, especially in bone, also affect its resilience and mechanical properties [5].
The diversity of collagen types allows your body to fine-tune tissue properties. For example, type II collagen is dominant in cartilage, giving joints their shock-absorbing qualities. Type III is found in blood vessels and skin, supporting elasticity and wound healing. The balance and structure of these different collagen types shift with age, activity, and disease.
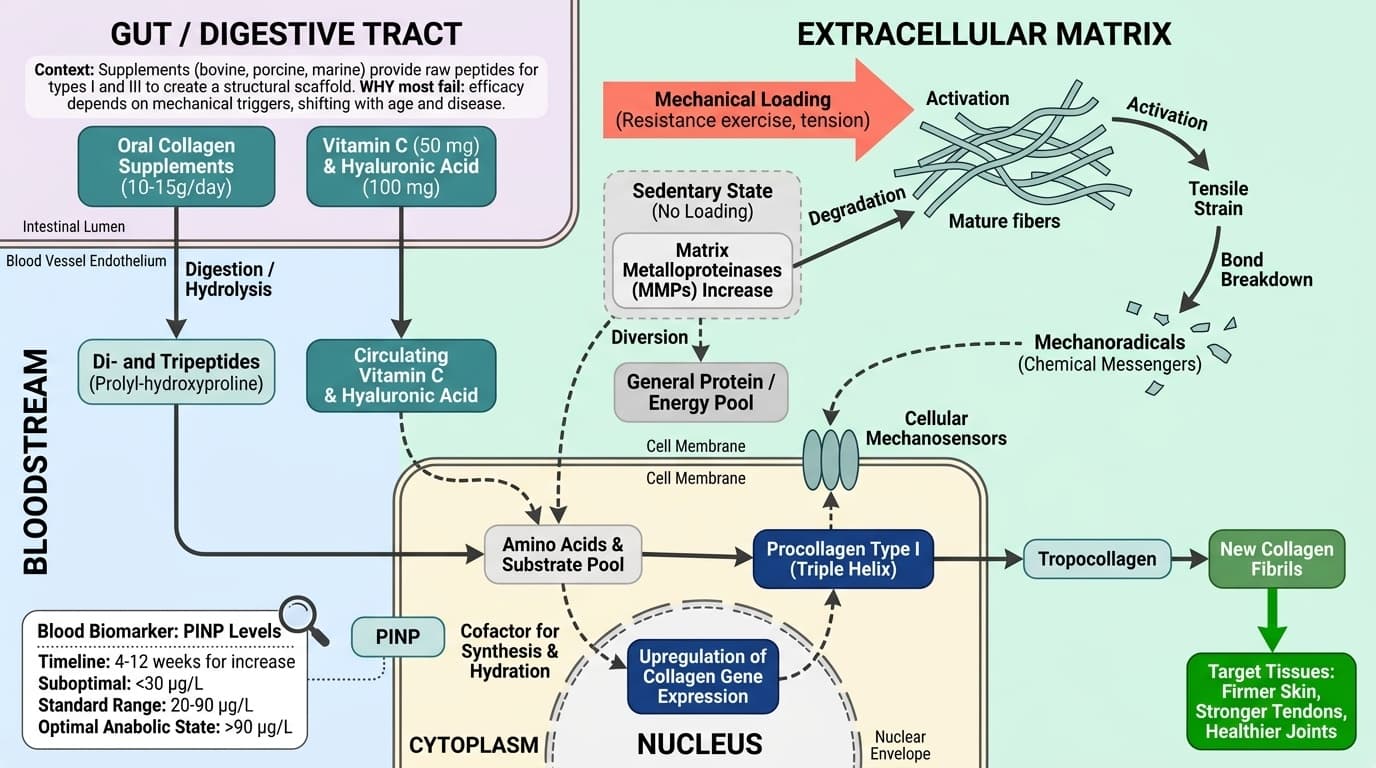
Most supplements on the market contain hydrolyzed collagen peptides—usually derived from bovine, porcine, or marine sources—that target types I and III. However, your body can only use these peptides if the underlying mechanical environment signals the need for repair or growth. Without that signal, the extra peptides are likely used as general protein or energy [1,3].
Understanding collagen’s structure and diversity sets the stage for why simply ingesting more isn’t enough. Next, you’ll see how your body actually builds and remodels collagen—and why mechanical stress is the real trigger.
Collagen production in your body is tightly regulated by signals from both your cells and your environment. The most powerful signal? Mechanical stress. When you load your tissues—whether through resistance exercise, stretching, or even postural tension—your cells sense these forces and respond by ramping up collagen synthesis [3,7].
Recent mechanobiology research has uncovered a fascinating process: when collagen fibers experience mechanical strain, some bonds break, generating 'mechanoradicals.' These molecular fragments act as chemical messengers, telling your cells to repair and reinforce the area with new collagen [15]. This response is highly localized—meaning only the tissues that experience stress signal for extra collagen production.
One 2025 review highlighted that without regular tensile loading, collagen turnover slows dramatically, and the body may even increase the activity of matrix metalloproteinases (MMPs), enzymes that break down collagen [7]. This explains why sedentary individuals lose tissue strength over time, while athletes or those engaged in regular resistance training maintain or even enhance their collagen matrix.
The timeline for detectable changes in collagen synthesis after starting a new loading regimen is about 4 to 12 weeks, depending on tissue type and intensity of exercise [7]. For example, PINP (procollagen type I N-terminal propeptide), a key blood biomarker of collagen formation, can rise by 20-40% after 8 weeks of consistent resistance training in adults. PINP's standard reference range is 20-90 µg/L, but optimal anabolic states for tissue repair are typically at the higher end or slightly above this range in active individuals.
The bottom line: mechanical loading is not optional if you want your collagen supplement to work. Next, we’ll look at the clinical evidence for collagen supplements—and why most studies show minimal effects without the right mechanical stimulus.
Collagen supplements are now available in countless forms—powders, capsules, gummies, and even drinks. Most products use hydrolyzed collagen peptides, which are small fragments produced by breaking down larger collagen molecules for easier absorption [1]. Some newer formulations include specific delivery technologies, like liposomal or nanoparticle encapsulation, to potentially improve bioavailability. But does any of this matter for real-world results?
Your body digests hydrolyzed collagen into di- and tripeptides, which can reach the bloodstream within hours. Studies show that after ingesting 10 grams of hydrolyzed collagen, blood levels of key peptides like prolyl-hydroxyproline peak in 1-2 hours and return to baseline by 6 hours [1]. However, this spike is not itself a guarantee of increased tissue collagen. The real bottleneck is whether your tissues demand more collagen—driven by mechanical loading, not just availability of raw materials.
The dose-response relationship is surprisingly flat above 10-15 grams per day. Multiple trials have found little additional benefit at 20 grams compared to 10 grams, especially in the absence of concurrent resistance exercise [1,3]. For skin and joint health, most studies use 10-12 grams daily, taken on an empty stomach for maximum absorption.
Form matters most for people with sensitive digestion (marine collagen may be less allergenic) or for specific stacking strategies. For example, combining collagen with 50 mg vitamin C and 100 mg hyaluronic acid enhances both absorption and utilization, as shown in a 2022 trial [1]. These cofactors support enzymatic crosslinking and tissue hydration, which are crucial for visible results.
Demographic note: Older adults, especially post-menopausal women, show a blunted response to collagen supplementation without exercise due to reduced mechanical signaling. Early warning signs of poor utilization include persistently low PINP (below 30 µg/L) and slow wound healing. Up next, let’s examine the clinical evidence—what works, what doesn’t, and why context is everything.
Despite the hype around collagen supplements, clinical evidence shows that benefits are highly dependent on your activity level and baseline tissue health. A 2024 meta-analysis of twelve trials found that collagen supplementation alone rarely leads to significant improvements in skin elasticity, joint pain, or bone density unless paired with regular physical loading [7].
The most consistent benefits are seen when collagen is combined with resistance exercise. For example, a 2023 RCT tracked two groups of women over 12 weeks: one took 15 grams of hydrolyzed collagen daily with a twice-weekly strength routine, while the other took collagen without exercise. Only the exercise group saw a significant rise in PINP (an average increase of 35 µg/L) and visible improvements in skin firmness and joint comfort. The supplement-only group’s results were indistinguishable from placebo [7].
Older adults face unique challenges. Aging tissues are less responsive to both mechanical and nutritional signals, likely due to changes in collagen crosslinking and reduced cell sensitivity [2,4]. In this population, stacking collagen with vitamin C and moderate resistance exercise has shown modest improvements in functional outcomes—such as grip strength and skin hydration—after 8-16 weeks [2]. However, the dose must be consistent, and the loading pattern should be progressive to keep signaling for new collagen.
Athletes and highly active people show the most robust response, especially in tendons and joints. In these groups, stacking 10-15 grams of collagen with vitamin C 30-60 minutes before exercise led to a significant increase in tendon stiffness and lower injury rates, as measured by imaging and functional tests [7].
For anyone, early warning signs of ineffective supplementation include no change in PINP or PICP (procollagen type I C-terminal propeptide), and persistent joint pain despite adherence. If this is your experience, it’s likely a mechanical—not nutritional—problem. Next, let’s get practical: which biomarkers should you track, and how can you interpret your progress?
Tracking your collagen health goes beyond watching for visible changes. The most informative way to assess your body’s collagen response is through blood biomarkers specific to collagen turnover. The three most studied are PINP (procollagen type I N-terminal propeptide), PICP (C-terminal propeptide), and CTX (C-terminal telopeptide of type I collagen) [7].
PINP reflects new collagen formation. For adults, the standard reference range is 20-90 µg/L, with optimal anabolic states typically between 60-120 µg/L during active tissue remodeling. PICP provides similar insights, but is less commonly available. CTX measures collagen breakdown; a high CTX (above 0.5 ng/mL) with low PINP suggests net tissue loss—a sign to increase mechanical loading or review your supplement stack.
What moves these markers? Regular resistance training will boost PINP by 20-40% within 8-12 weeks. Vitamin C intake (at least 50 mg alongside collagen) enhances this effect by supporting enzymatic crosslinking [1]. Inflammation, inactivity, or high MMP activity (matrix metalloproteinases) can suppress PINP and raise CTX, indicating tissue breakdown [7].
Demographic context matters. Post-menopausal women and older men often have lower baseline PINP, so a rise of even 10-15 µg/L may be significant. Athletes, especially those in tendon-heavy sports, tend to have higher PINP and lower CTX. Interaction effects: high vitamin D status (>40 ng/mL) and sufficient protein intake (>1.2 g/kg/day) further optimize collagen synthesis and marker movement.
Early warning signs: If you see persistently low PINP (below 30 µg/L) or a rising CTX despite proper supplementation and exercise, investigate for underlying inflammation or protein malnutrition. Now that you know how to measure success, let’s explore how you can maximize collagen gains with smart stacking and timing.
Collagen supplements are most effective when paired with key cofactors and interventions that drive your body to use them. Mechanistically, vitamin C is essential for the hydroxylation of proline and lysine—critical steps in collagen crosslinking and stability [1]. Without enough vitamin C, much of the ingested collagen is wasted. A 2022 clinical trial showed that taking 50-100 mg vitamin C with 10 grams of collagen boosted PINP by an additional 15% over collagen alone [1].
Hyaluronic acid, at doses of 100-200 mg daily, supports tissue hydration and further enhances visible skin improvements when combined with collagen. Some supplement blends include both, and this stacking has been linked to higher skin elasticity scores after 8-12 weeks [1].
Timing matters. Studies indicate that taking collagen (plus cofactors) 30-60 minutes before resistance training maximizes uptake and utilization in loaded tissues. The mechanism: exercise increases blood flow to stressed tissues, delivering more of the needed peptides and vitamins right when your cells are signaling for repair [7].
Other interventions with possible synergy: glycine and proline supplementation can support endogenous collagen production, especially in older adults. Maintaining high protein intake (at least 1.2-1.5 g/kg/day) ensures a sufficient amino acid pool. For skin, adding antioxidants like astaxanthin (4 mg daily) may protect existing collagen from UV damage and further improve outcomes.
Demographic-specific note: Active individuals and those recovering from injury see the largest benefit from stacking, while sedentary adults may see little effect unless they add mechanical loading. If you want to maximize results, build your stack around both supplementation and stimulus. In the next section, we’ll look at how different demographics respond to these strategies.
Not everyone responds to collagen supplementation in the same way. Age, gender, and lifestyle profoundly affect both your baseline collagen status and your body’s ability to build new tissue. For example, older adults—and especially post-menopausal women—experience slower collagen synthesis due to hormonal changes and reduced mechanical signaling [2,4].
In this group, stacking 10-15 grams of hydrolyzed collagen with 50-100 mg vitamin C and moderate resistance training (2-3 times per week) led to modest but significant increases in skin elasticity and grip strength after 12 weeks. The timeline to see changes is generally slower—about 12-16 weeks compared to 8-12 weeks in younger adults. Early warning signs of poor response include slow wound healing, persistent joint pain, and stagnant PINP or PICP despite adherence.
Men generally have higher baseline collagen density and respond more quickly to both supplementation and exercise, likely due to higher mechanical loading and testosterone-driven tissue turnover. However, sedentary men over 50 still experience rapid collagen loss if they do not maintain regular loading patterns. In both genders, inactivity, chronic inflammation, or low protein intake blunt the benefits of supplementation.
Athletes and highly active individuals see the greatest gains, especially when timing supplements before workouts. For example, tendon adaptation in runners improved measurably (lower injury rates, higher ultrasound-measured stiffness) when collagen and vitamin C were combined with structured loading [7]. Conversely, those with chronic disease or high levels of inflammation may need to address underlying factors before seeing significant collagen gains.
Understanding these demographic nuances lets you tailor your intervention for maximum effectiveness. Next, we’ll address common myths and misconceptions about collagen—and what the science really says.
Collagen supplement marketing is full of big promises, but science tells a more nuanced story. One of the most persistent myths is that simply eating more collagen will directly translate to better skin, stronger joints, or thicker hair. In reality, your body treats collagen peptides like any other protein—unless you combine them with the right triggers for tissue-specific remodeling [1,3,7].
Another misconception is that all forms of collagen are equally effective. Most supplements use hydrolyzed collagen, which is well absorbed but not targeted to specific tissues. The idea that marine collagen is inherently superior is not supported by human trials—though it may have a lower allergenic potential for some people [1].
Some believe that high-dose collagen (20-30 grams daily) offers extra benefit, but studies consistently show that 10-15 grams is the practical upper limit for absorption and utilization, especially when paired with mechanical loading. Taking more simply increases your protein intake, not your collagen synthesis [1].
Finally, many overlook the crucial role of cofactors like vitamin C, or the need for progressive resistance exercise. Without these, most of the supplement is used as general protein or energy, not for new tissue construction. Early warning sign: if you’ve taken collagen for months with no visible or measurable results (no change in skin, joint comfort, or PINP), you’re likely missing the essential mechanical component.
With these myths addressed, you can move forward with a science-based strategy that actually works. In our final section, we’ll bring all the evidence together into a practical action plan for optimizing your collagen system.
To get the best out of your collagen supplement, you need a protocol that combines nutrition, timing, and mechanical loading. For most adults, the evidence-based approach is as follows: take 10-15 grams of hydrolyzed collagen with 50-100 mg vitamin C and 100 mg hyaluronic acid, 30-60 minutes before resistance exercise three times per week [1,7]. This protocol is supported by multiple trials showing significant improvements in collagen biomarkers (like PINP), skin elasticity, and joint health.
Track your progress by measuring PINP and CTX every 8-12 weeks. If PINP rises by at least 10-20 µg/L and CTX remains stable or decreases, you’re in an anabolic state. If not, review your loading pattern and adjust your supplement stack. For older adults or those recovering from injury, consider adding glycine and proline, and ensure your total protein intake is above 1.2 g/kg/day.
Synergies matter: keep vitamin D above 40 ng/mL and control inflammation to maximize response. If you see early warning signs—such as slow healing or no marker movement—revisit your exercise intensity or check for hidden inflammation. Demographic adjustments: older women may need a longer ramp-up period (12-16 weeks) and more frequent loading sessions, while athletes can benefit from higher loading intensity.
Looking ahead, research into personalized collagen protocols—using genetic markers and advanced biomarker tracking—may allow even more tailored interventions. But the core message is clear: supplements alone are not enough. Collagen is a dynamic, mechanically responsive system. To make your supplements work, make your body use them. This is the frontier of mechanobiology and targeted supplementation.
Why Your Collagen Supplement Probably Isn't Working (And How to Tell)
The New Science of Mechanobiology and Collagen Response
Diagram glossary
- bovine:
- Relating to cattle, often used to describe a primary source of dietary collagen supplements.
- Collagen:
- The primary structural protein forming the backbone of skin, bones, tendons, and ligaments.
- hydroxyproline:
- An amino acid unique to collagen that stabilizes its triple-helix structure.
- III:
- A specific type of structural collagen commonly found alongside type I in connective tissues.
- marine:
- Relating to the sea, commonly referring to collagen sourced from fish or aquatic life.
- MMP:
- An enzyme family, known as matrix metalloproteinases, responsible for degrading extracellular matrix proteins.
- PINP:
- A procollagen cleavage product measured in blood as a biomarker of new collagen synthesis.
- porcine:
- Relating to pigs, which serve as a common biological source for extracted collagen.
- procollagen:
- The precursor molecule to collagen that is secreted by cells before final assembly.
- propeptide:
- An amino acid sequence cleaved from a precursor protein to make it fully functional.
Conclusions
The real driver of collagen health is not the supplement itself, but how your body is challenged to use it. Collagen supplements, especially hydrolyzed peptides, can provide the raw materials, but only regular mechanical loading—like resistance exercise—signals your body to build new collagen fibers. Measuring specific biomarkers (such as PINP and CTX) gives you a feedback loop to track your progress and optimize your protocol. Stacking collagen with vitamin C, hyaluronic acid, and supporting nutrients further amplifies results, especially when timed before physical loading. Tailor your approach to your age, gender, and activity level for the best outcomes. The evidence is clear: if you want your collagen supplement to actually work, you must pair it with purposeful, progressive mechanical stress.
Most clinical studies on collagen supplements are still short-term (8-16 weeks) and often combine multiple interventions, making it hard to isolate the effect of collagen alone. There are few large, long-term RCTs in diverse populations, especially older adults and those with chronic disease. Biomarker reference ranges may vary by lab, and not all tests are widely available. Individual response can vary due to genetics, baseline tissue health, and unmeasured factors like inflammation or micronutrient status. Future research should focus on personalized protocols, longer timelines, and direct measurement of tissue remodeling using advanced imaging.
Track this in your stack
See how collagen relates to your health goals and monitor changes in your biomarkers over time.