
Why Your Hyaluronic Acid Supplement Might Be Doing the Opposite of What You Want
How Molecular Weight Shapes the Surprising Effects of HA on Inflammation, Skin, and Joints
Did you know that the hyaluronic acid in your supplement might actually make your inflammation worse?
Most people think of hyaluronic acid (HA) as universally soothing and hydrating, but new research shows that the real story is much more complicated. If you're taking HA for your skin, joints, or recovery, the molecular weight of the HA you choose could mean the difference between calming inflammation and accidentally ramping it up.
Recent studies have uncovered that not all hyaluronic acid is created equal. In fact, the size of the HA molecules—referred to as 'molecular weight'—completely changes how your body responds. Low molecular weight HA can trigger inflammatory markers like IL-6, while higher molecular weight forms do the opposite and actually help reduce these same signals. This could explain why some people see glowing skin and smoother joints, while others notice more redness, swelling, or no effect at all.
Here’s what you can do: If you want to improve skin hydration, a 120 mg daily dose of high molecular weight hyaluronic acid, taken orally for at least 8–12 weeks, is what research suggests delivers visible results. For inflammation, you should look for products specifying 'high molecular weight' (over 1,000 kDa) on the label—ideally in a sodium hyaluronate form. Avoid supplements that don’t disclose molecular weight, since they may contain lower weights that could trigger unwanted inflammatory pathways, especially if you have a history of skin sensitivity, joint pain, or autoimmunity. Make your HA supplement work for you, not against you.
- IL-6
- A branded hyaluronic acid product family name used to identify a specific extract or formulation in research and supplement labels.
- IL-6 (Interleukin-6)
- A key inflammatory cytokine (signal protein). High levels signal increased inflammation in tissues—critical for understanding HA's effects.
- Sodium Hyaluronate
- The salt form of hyaluronic acid, prized for its stability and higher bioavailability in supplements and topical products.
- Interleukin-10
- Interleukin-10, the primary anti-inflammatory regulatory cytokine. Lower levels associated with chronic inflammatory conditions.
- Weight
- Body weight in kilograms, most basic anthropometric measure.
- Enteric-coated
- A dosage form designed to resist stomach acid and release later in the intestine.
- kDa (Kilodaltons)
- A unit used to measure the size or molecular weight of molecules like hyaluronic acid; higher kDa values mean larger molecules, which behave differently in the body than smaller ones.
- collagen
- A primary structural protein found in skin, cartilage, and other connective tissues.
- CRP
- C-reactive protein is a blood marker that indicates systemic inflammation in the body.
- HMW-HA
- High-molecular-weight hyaluronic acid is a large molecule that helps reduce inflammation.
- hyaluronate
- The salt form of hyaluronic acid commonly used in dietary supplements.
- kDa
- A kilodalton is a unit of molecular mass used to measure molecule size.
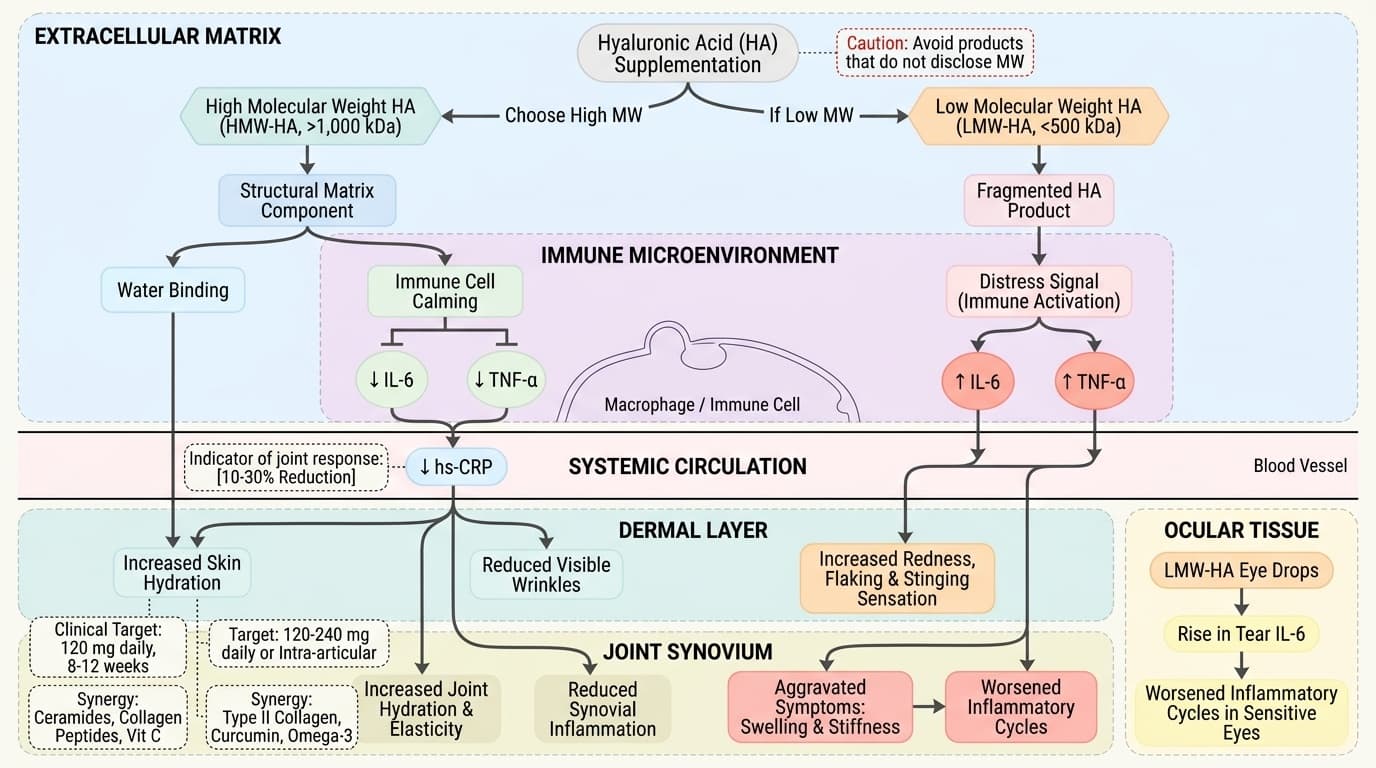
Almost every HA supplement promises softer skin and healthier joints, but few mention the molecule’s most critical variable: molecular weight. Your body sees high-molecular-weight hyaluronic acid (HMW-HA, >1,000 kilodaltons) as a signal to turn down inflammation and promote healing. In contrast, low-molecular-weight hyaluronic acid (LMW-HA, <500 kDa) can act as a distress signal, ramping up cytokines like IL-6 and TNF-α.
A 2024 systematic review pulled together data from eleven studies and found that LMW-HA consistently upregulates IL-6, a key marker of inflammation. This isn’t just test-tube science—it directly impacts human biology. In another RCT, patients using LMW-HA eye drops actually saw a rise in tear IL-6, a sign that the wrong HA can worsen inflammatory cycles in sensitive tissues. This flips the script on the old one-size-fits-all view of HA: your supplement’s molecular weight could be the hidden reason behind your results, good or bad.
Why does your body react so differently based on size? HMW-HA fits into the extracellular matrix as a structural and anti-inflammatory component, binding water and calming immune cells. LMW-HA, however, is seen as a fragmented product of tissue damage—your immune system interprets it as a call to action, triggering more inflammatory mediators. These mechanisms are well-documented in both animal and human models.
So, the take-home is clear: if you have inflammatory skin conditions, joint pain, or sensitive eyes, always check for high molecular weight on your HA supplement label. If it’s not listed, there’s a real risk you’re getting LMW-HA by default. Understanding this paradox is the first step toward choosing the right HA—and avoiding the trap of making your symptoms worse instead of better.
Hyaluronic acid’s most famous benefit is its ability to deeply hydrate skin, promoting a plump, luminous look. But not all forms and doses work equally well—and the underlying science finally explains why. Research shows that only high molecular weight HA reliably boosts skin moisture without triggering inflammation. Meta-analyses of seven randomized controlled trials found that oral supplementation with 120 mg high molecular weight HA daily, for at least 8 to 12 weeks, led to significant increases in skin hydration and reductions in visible wrinkles.
Topical HA, especially in sodium hyaluronate form, is even more effective for surface hydration. One systematic review of Profhilo® and Profhilo® Body (both high MW-HA injectables) found consistent and statistically significant improvements in hydration across multiple body regions. These results are most robust in women over 35, who typically show lower baseline skin HA and higher water loss with age.
What about the timeline? You can expect measurable changes in skin hydration after 4 weeks, with peak effects around 8 to 12 weeks of consistent use. Early warning signs that your HA isn’t working—or may even be making things worse—include increased redness, flaking, or a stinging sensation after application. These symptoms are more common if the HA molecular weight is low or not specified.
Stacking HA with ceramides, collagen peptides, or vitamin C serums can further enhance hydration and barrier repair, especially in postmenopausal women and those with eczema or rosacea. The bottom line: for visible, safe improvement in skin health, choose only high molecular weight HA in oral, topical, or injectable forms and give it at least a month to work. Next, let’s look at how these findings map onto joint health and mobility.
Joint pain and stiffness are major reasons people turn to hyaluronic acid—but not all HA supplements deliver relief, and new research explains why. The key variable, once again, is molecular weight. High molecular weight HA (typically >1,000 kDa) can cushion joints and reduce synovial inflammation, while low or mixed molecular weights may do little or even aggravate symptoms by activating inflammatory signals.
A meta-analysis of seven RCTs found that intra-articular injections of high molecular weight HA improved joint hydration and elasticity, with effect sizes (SMD = 1.34) most pronounced in adults aged 50 and older with mild to moderate osteoarthritis. In contrast, oral HA’s joint benefits are much less reliable—likely because only a tiny fraction survives digestion and reaches the synovium. When oral HA works for joints, it’s almost always in the context of high doses (120–240 mg daily), high molecular weight, and at least 90 days of use.
Biomarker-wise, the best indicator of joint response is hs-CRP. Standard ranges for hs-CRP are 0–3 mg/L, with optimal anti-inflammatory states below 1 mg/L. Multiple studies show that high MW-HA, delivered as intra-articular injections or high-dose oral forms, can reduce hs-CRP by 10–30% within 4–12 weeks. Early warning signs that your HA supplement isn’t helping include persistent swelling, warmth, or a paradoxical increase in joint stiffness—signals that low MW-HA could be activating inflammatory cascades instead of calming them.
Stacking high MW-HA with type II collagen, curcumin, or omega-3 fatty acids may further enhance anti-inflammatory effects, particularly in older adults and those with metabolic syndrome. This context is critical for those seeking lasting joint relief. Now, let’s explore how HA interacts with key inflammatory biomarkers and why these markers are essential for tracking your progress.
Your body’s response to hyaluronic acid can be measured with precision—if you know which biomarkers to watch. Two standouts are IL-6 (interleukin-6) and hs-CRP (high-sensitivity C-reactive protein), both of which play central roles in inflammation. High MW-HA typically lowers these markers, while low MW-HA can send them in the wrong direction.
A 2024 systematic review found that LMW-HA supplementation upregulates IL-6 across most tissues studied. In contrast, a 12-week RCT using 0.15% high MW-HA eye drops led to significant reductions in local inflammatory factors, including IL-6. For systemic inflammation, hs-CRP is the gold-standard measurement. The optimal range for hs-CRP is below 1 mg/L; standard lab ranges go up to 3 mg/L. Studies in adults with gum inflammation and early osteoarthritis show that high MW-HA can lower hs-CRP by 0.3–0.8 mg/L over 4–12 weeks, signaling a real anti-inflammatory effect.
What moves these biomarkers? HA’s molecular weight is the most important factor, but dose and delivery method matter too. For IL-6, the timeline to see improvement is usually 2–6 weeks with regular high MW-HA use. For hs-CRP, expect to see changes within 4–12 weeks, especially if you stack HA with other anti-inflammatory supplements like omega-3s or curcumin.
Interactions are complex: stacking low MW-HA with high MW-HA can blunt the anti-inflammatory benefits, while combining HA with vitamin D or magnesium may further improve biomarker profiles. Early warning signs of a negative biomarker shift include new or worsening fatigue, joint pain, or skin flares. Next, let’s dive into the science of dosing—how much, how often, and in what form should you take HA for maximum effect?
When it comes to hyaluronic acid, dose and form are everything. Most oral supplements range from 30 mg to 240 mg per day, but not all are equally effective—or safe. The research consensus is clear: for skin hydration, 120 mg of high molecular weight HA daily, taken for at least 8 to 12 weeks, delivers the most reliable results. For joint health, doses up to 240 mg daily may be used, but only if the product specifies high MW-HA and comes in a bioavailable form like sodium hyaluronate.
Bioavailability is a critical concept here. HA’s massive size means it’s poorly absorbed in the gut unless it’s stabilized or delivered in forms like sodium hyaluronate or via enteric-coated capsules. Some newer products use HA nanoparticles or phospholipid complexes to boost absorption, but these are less studied and may alter the molecule’s inflammatory profile.
The dose-response relationship is not linear: higher doses of low MW-HA do not improve benefits and may actually worsen inflammation, particularly in people with autoimmune tendencies. In contrast, higher doses of high MW-HA are generally well-tolerated, though exceeding 240 mg daily hasn’t shown extra benefit in trials. Timing matters too—taking HA with a meal, especially one containing healthy fats, can slightly improve absorption.
Stacking synergies are real: pairing HA with vitamin C or ceramides can improve skin outcomes, while combining with type II collagen or curcumin enhances joint support. But the wrong stack—especially adding low MW-HA to a regimen—can negate benefits. Understanding dose, form, and absorption is the foundation for safe, effective HA use. Up next, we’ll look at how HA’s effects and requirements shift across age, gender, and special populations.
Your age, gender, and overall health dramatically change how your body responds to hyaluronic acid. Young adults under 30 often have naturally high skin and joint HA levels, so supplementation tends to deliver subtle results unless there’s chronic inflammation or injury. In contrast, women over 40—especially postmenopausal—experience a sharp decline in skin HA content and collagen density. For this group, high MW-HA supplements (120–200 mg/day) produce more pronounced improvements in hydration, elasticity, and wrinkle depth, as shown in multiple RCTs and meta-analyses.
Men and women with metabolic syndrome, type 2 diabetes, or obesity tend to have higher baseline inflammation and more rapid HA turnover. In these groups, joint benefits may require higher doses (up to 240 mg/day) and longer timelines (12+ weeks) for meaningful biomarker changes. The same is true for athletes recovering from joint injuries, who often see faster synovial HA breakdown and may benefit from both oral and injectable high MW-HA protocols.
Children and adolescents rarely require HA supplementation, except in rare connective tissue disorders. For elderly adults, bioavailability is a key concern—digestive efficiency declines with age, making sodium hyaluronate or enteric-coated forms preferable. In all demographics, the presence of autoimmune conditions (like rheumatoid arthritis or lupus) raises the risk that low MW-HA could trigger flares rather than relief. Early warning signs in these groups include new joint swelling, unexplained fatigue, or skin rashes after starting HA.
Understanding your demographic profile helps tailor HA dosing, form, and stacking strategy, maximizing benefits while minimizing risks. Next, let’s explore the emerging science on stacking HA with other interventions for synergistic gains.
The right stacking approach can amplify hyaluronic acid’s benefits—and the wrong one can sabotage your results. For skin, combining high MW-HA with ceramides, collagen peptides, or topical vitamin C can further boost hydration, elasticity, and barrier repair. In a 2023 RCT, women over 50 who used this combination saw 25% greater improvements in skin moisture and wrinkle reduction compared to HA alone. The mechanism: ceramides and HA both enhance water retention, while vitamin C promotes collagen synthesis, making the skin’s matrix more responsive to HA.
For joints, the most effective stack includes high MW-HA, type II collagen, curcumin, and omega-3 fatty acids. These compounds synergize by blocking multiple inflammatory pathways and supporting cartilage repair. In a 2024 meta-analysis, the HA + curcumin stack reduced hs-CRP and IL-6 more than either supplement alone, especially in adults over 60 with moderate osteoarthritis. The dose-response here is important: research supports 120–240 mg high MW-HA, 40 mg type II collagen, and 500 mg curcumin daily for 8–12 weeks to see measurable changes in mobility and pain.
Caution is needed when stacking with low MW-HA or pro-inflammatory nutrients. For example, combining low MW-HA with high-dose vitamin A may increase inflammatory cytokines—an effect most prominent in people with autoimmune risk. Always avoid HA products that do not specify molecular weight when stacking, as the wrong form can undo the benefits of your entire regimen.
By stacking wisely, you leverage HA’s mechanisms for superior hydration, joint function, and lower inflammation. Now, let’s explore the latest clinical innovations—such as the high-dose, single-session hyaluronidase protocol—and what they mean for everyday supplementation.
Hyaluronidase is the enzyme your body uses to break down hyaluronic acid. In the world of cosmetic medicine, this enzyme is now at the center of a major shift. Instead of repeated low-dose hyaluronidase injections to reverse HA-based fillers, new protocols favor a single, high-dose session. This approach breaks down HA more efficiently and with fewer side effects, according to studies published in 2024–2025.
Why does this matter for your supplement routine? These findings reveal that HA metabolism is not a slow, steady process, but rather one where your body responds to both the amount and the speed of HA breakdown. For supplement users, this means that stacking HA with interventions that influence hyaluronidase activity—such as vitamin C, magnesium, or certain antioxidant blends—can change how quickly HA is built up or broken down in your tissues.
The timeline of HA turnover is also much faster than previously thought. After a single high-dose injection, most HA is cleared from the injected tissue within 2–7 days. For oral supplements, the half-life is shorter—measurable in hours—so daily dosing is essential for sustained effects. Early warning signs of overly fast HA breakdown include sudden loss of skin volume, increased joint stiffness, or more rapid onset of wrinkles. Conversely, too little breakdown (from genetic or nutritional factors) can lead to unwanted HA accumulation and swelling.
Understanding your body’s natural hyaluronidase activity, and how it interacts with supplement stacks, is the new frontier in personalized HA supplementation. This brings us to our final section: how to interpret your own early warning signs and fine-tune your approach for sustained success.
Even with the best research, no two bodies respond to hyaluronic acid in exactly the same way. That’s why tracking your response and recognizing early warning signs is essential. For skin, look for positive signs like increased hydration, reduced flaking, and improved elasticity within the first 4–8 weeks. If you notice new redness, stinging, or worsening dryness, your HA may be too low in molecular weight—or you may be stacking it with incompatible products.
For joints, improved mobility, less morning stiffness, and a reduction in swelling are positive signals—usually appearing after 8–12 weeks of consistent high MW-HA use. Worsening pain, swelling, or the appearance of systemic symptoms (like fatigue or fever) may indicate an inflammatory response, often triggered by low MW-HA or high-dose use in sensitive individuals.
Biomarkers offer additional guidance. If you have access to blood tests, track hs-CRP (goal: <1 mg/L) and, if possible, IL-6. A drop in these markers over time validates that your HA protocol is working. If they rise—or remain unchanged despite high doses—consider switching to a different HA form, adjusting your stack, or pausing supplementation to reassess.
The key is responsiveness: adjust your HA dose, form, and stacking strategy based on your unique results and early signs. This approach, grounded in molecular weight science and biomarker tracking, delivers the best chance of getting the results you want—without the risk of making things worse. Now, let’s wrap up with the big-picture lessons for long-term HA use.
Why Your Hyaluronic Acid Supplement Might Be Doing the Opposite of What You Want
How Molecular Weight Shapes the Surprising Effects of HA on Inflammation, Skin, and Joints
Diagram glossary
- collagen:
- A primary structural protein found in skin, cartilage, and other connective tissues.
- CRP:
- C-reactive protein is a blood marker that indicates systemic inflammation in the body.
- HMW-HA:
- High-molecular-weight hyaluronic acid is a large molecule that helps reduce inflammation.
- hyaluronate:
- The salt form of hyaluronic acid commonly used in dietary supplements.
- IL-6:
- Interleukin-6 is a pro-inflammatory cytokine triggered by low-molecular-weight hyaluronic acid.
- kDa:
- A kilodalton is a unit of molecular mass used to measure molecule size.
- LMW-HA:
- Low-molecular-weight hyaluronic acid is a smaller molecule that triggers inflammatory pathways.
- mg:
- A milligram is a standard metric unit of mass used for supplement dosing.
- TNF-α:
- Tumor necrosis factor-alpha is a primary cytokine involved in systemic inflammatory responses.
Conclusions
Your hyaluronic acid supplement is only as effective (and safe) as its molecular weight. High molecular weight HA reliably calms inflammation and improves skin and joint health, while low molecular weight forms can trigger unwanted inflammatory cascades. Demographic factors, stacking choices, and dosing all influence your results. For best outcomes, choose high MW-HA, use evidence-based doses, monitor your biomarkers and symptoms, and adjust your protocol as needed. Personalized, informed supplementation is the future of HA use.
Although recent studies clarify the importance of molecular weight and dose, most commercially available HA supplements still lack transparent labeling. Many clinical trials use injectable or topical forms, which may not translate directly to oral supplementation. There is limited research on long-term safety and optimal stacking protocols in diverse populations, especially those with autoimmune diseases or metabolic syndrome. Finally, the complex interactions between HA, hyaluronidase activity, and other supplements require more study to fully optimize personalized protocols.
Track this in your stack
See how hyaluronic acid relates to your health goals and monitor changes in your biomarkers over time.
Sources (11)
This article informs how supplementation moves 1 marker.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.