
Why Your Iron Supplement Dose May Not Matter—But Your Hepcidin Level Does
How your body's iron gatekeeper determines whether any dose works at all
You might think taking more iron will fix low energy, brain fog, or feeling run down.
But the real gatekeeper for iron is not your supplement dose—it is a hormone called hepcidin. Your body decides how much iron gets absorbed, and piling on higher doses often does nothing if hepcidin is working against you. Let’s dig into how this works and what you can actually do, so your iron strategy is guided by science, not guesswork.
- IL-6 (Interleukin-6)
- An inflammation signal that can raise hepcidin. It is a cytokine, not an iron product name.
- Hepcidin
- A liver hormone that can block iron from entering your blood by shutting down iron transport.
- Elemental iron
- The usable iron amount on the label (not the pill’s total weight). Example: 325 mg ferrous sulfate has about 65 mg elemental iron.
- Serum iron
- A blood test for iron moving in your blood right now. It can change fast.
- Ferritin
- Ferritin, the primary iron storage protein reflecting total body iron stores.
- TIBC (Total Iron Binding Capacity)
- A blood test that helps interpret TSAT and serum iron. It often rises when iron is low.
- CRP (C-reactive protein)
- A common inflammation blood test. Higher CRP often means higher hepcidin and lower iron absorption.
- CRP
- A blood test marker used to detect and measure inflammation in the body.
- ferroportin
- The primary iron exporter protein located in the gut and storage cells.
- IL-6
- A marker of inflammation that can be tested if iron levels do not rise.
Imagine standing in the supplement aisle, holding a bottle of iron. You feel tired. Maybe you are looking for a fix for that mid-afternoon fog, or your doctor mentioned your bloodwork was off. The label says one hundred twenty-five milligrams, but next to it is another bottle with two hundred. Your first instinct is to think, maybe more is better. Maybe a higher dose will get you back to normal faster.
But here is the twist. For many people, higher doses of iron do not work better. In fact, sometimes they do not work at all. You could take two or even three times the recommended amount and still end up with low energy, brain fog, or stubborn anemia on your next blood test. The problem is not you. It is not even the supplement. The real story is happening inside your body, controlled by a hormone you have probably never heard of: hepcidin.
Hepcidin is like a security guard at the gate of your gut. No matter how much iron you swallow, if the guard says stop, almost nothing gets through. This is why so many people are frustrated when their iron numbers do not budge—or when they get all the stomach upset and none of the benefit. The answer is not always to take more. The answer is to work with your biology, not against it.
So how does your body decide when to let iron in? And what can you do if you feel like your tank is always running on empty? Let’s unpack the science, then translate it into a plan you can actually use.
Iron is not just about your blood. It plays a starring role in how well your brain works, how balanced your hormones feel, and how strong your immune system stays. If your iron is low, you might notice more than just feeling tired—you might find it hard to focus, feel down or anxious, or get sick more easily.
Let’s start with your brain. Iron is central to making dopamine and serotonin, the chemicals that help you concentrate, stay motivated, and keep your mood steady. If you do not have enough iron, your brain cannot make or use these neurotransmitters efficiently. That is why iron deficiency often looks like trouble focusing, low motivation, or even depression—long before you ever become anemic.
For hormones, iron is critical at every age, but especially for women during their reproductive years. Monthly cycles, pregnancy, and even perimenopause can all drain iron stores. Low iron can worsen the fatigue, brain fog, and mood swings that show up with hormonal shifts. If you are on hormone therapy, your iron needs may change. For men and anyone past menopause, iron loss slows down, but the need for efficient iron use in hormone and energy metabolism remains.
Your immune system also depends on iron. White blood cells use iron to multiply and mount an effective response to infections. But here is the catch—when you are sick or inflamed, your body raises hepcidin intentionally, locking down iron to keep it away from invading bacteria. This defense mechanism keeps you safe during short-term illness, but if inflammation is chronic—like with obesity, autoimmune conditions, or metabolic syndrome—your iron can get stuck in storage and unavailable for use. That is why you can have plenty of iron on paper, but still feel tired and get sick often.
So what does all this mean? Iron status is about much more than preventing anemia. It is about keeping your brain sharp, your hormones balanced, and your immune defenses strong. But your body is always making tradeoffs—sometimes locking away iron to fight infection or inflammation, and sometimes opening the gates when it senses you need more. Understanding this balance is the key to real-world results.
If you have ever had a basic blood panel, you have probably seen ferritin on your results. Ferritin is your iron storage protein. When it is low, your body’s iron tank is running dry. But here is the catch—ferritin can be tricky. It goes up whenever you have inflammation, infection, or even after a tough workout. That means a "normal" ferritin does not always mean you have enough iron for your body to use.
What should you look at instead? There are three numbers that tell you the real story: serum iron, transferrin saturation, and ferritin—together.
Serum iron measures the amount of iron floating in your bloodstream right now. Transferrin saturation, or TSAT, tells you how much of your iron-carrying protein (transferrin) is actually loaded up with iron. Ferritin shows the backup supply. But if inflammation is in play, ferritin can look normal or even high, masking a real shortage.
Here is what the numbers mean for most adults:
Ferritin: You want at least thirty micograms per liter for basic health, but many experts suggest aiming for fifty to one hundred for optimal brain and hormone function, especially in women of childbearing age. Above two hundred micograms per liter may signal overload or hidden inflammation.
Serum iron: The typical range is sixty to one hundred seventy micograms per deciliter, but lower levels can be normal in the morning or after fasting. What matters is if your number is consistently at the low end, especially with low TSAT.
Transferrin saturation (TSAT): You want TSAT above twenty percent. Below that, your tissues are likely not getting enough active iron. For many people, twenty-five to thirty-five percent is a healthy range. Above forty-five percent could mean iron overload or a rare transport issue.
Total iron binding capacity (TIBC): This measures how much room there is for iron to bind. High TIBC with low iron means you are depleted. Low TIBC can show up in chronic disease.
If you suspect inflammation is muddying the waters, look at C-reactive protein (CRP) and interleukin-6 (IL-6). High CRP or IL-6 means your ferritin might be falsely elevated. In this case, focus more on TSAT and serum iron, and talk with your doctor about treating the underlying inflammation first.
A massive randomized trial in people with heart failure showed that changes in serum iron and TSAT over six months were better predictors of energy, brain function, and overall health than ferritin alone. That means watching these numbers over time gives you a far better sense of whether your iron plan is working. That brings us to what you can actually measure and do.
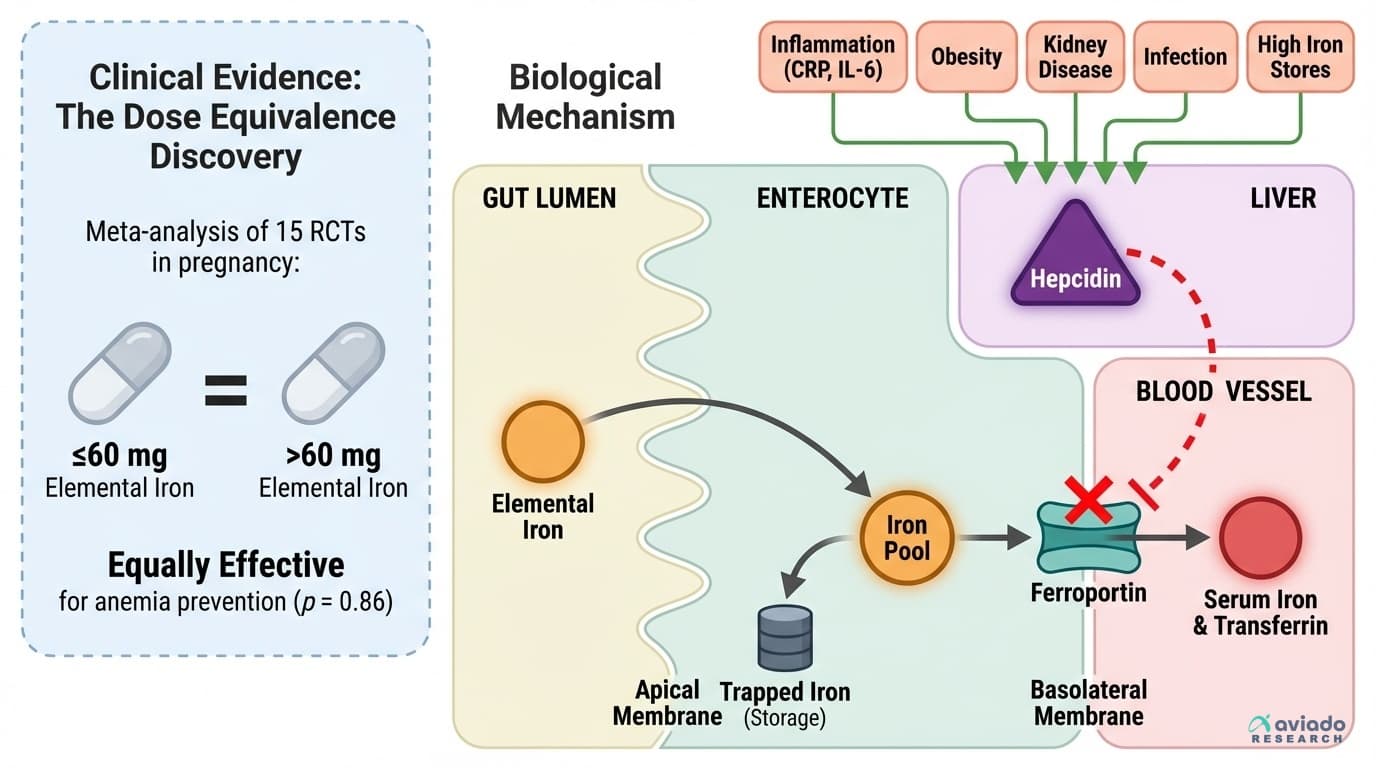
Here is where conventional wisdom often goes wrong. For decades, the advice was simple: take more iron. Many supplements come in one hundred to two hundred milligram doses, and people assume that higher means faster results. But a landmark meta-analysis of fifteen randomized trials in pregnant women found that daily doses at or below sixty milligrams of elemental iron worked just as well as higher doses to prevent anemia. In fact, once you cross that threshold, the only thing that goes up is the risk of stomach side effects.
So why does more not help? It comes back to hepcidin. This hormone, made by your liver, senses when your body is inflamed, infected, or already has enough iron. When hepcidin rises, it locks down a protein called ferroportin, which acts as the door for iron to leave your gut and storage sites. With high hepcidin, you could take as much iron as you want, and almost none of it gets in. It just passes through, often causing nausea or constipation along the way.
What is the protocol that works with your biology? Start with sixty milligrams of elemental iron once daily. This matches the evidence—and is the amount in a standard three hundred twenty-five milligram tablet of ferrous sulfate, which contains about sixty-five milligrams of usable iron. Take your iron away from calcium, tea, and coffee, all of which block absorption. Many people do best taking it on an empty stomach, though food may be needed if nausea is a problem.
Stick with your chosen dose for eight to twelve weeks, then recheck labs. If your serum iron and TSAT have not improved, do not just double the dose. Instead, ask about checking your CRP and IL-6. If inflammation is high, you may need to treat that first, or you may be a candidate for intravenous iron, which skips the gut gate entirely and delivers iron straight into your bloodstream. This protocol is not just about numbers—it is about respecting the body’s control system and using the right lever for your situation.
So what does the evidence say about the other factors that can make or break absorption? That is next.
Iron is not just about what supplement you pick. Your daily habits can make or break your absorption and your overall iron status. Here is how it works.
First, your diet. Heme iron, found in animal foods like red meat, poultry, and fish, is much more easily absorbed than non-heme iron from plant sources like beans, lentils, and spinach. If you are vegetarian or vegan, you can absolutely meet your needs, but you have to be more strategic. Pair non-heme iron sources with vitamin C-rich foods—think citrus, bell peppers, or strawberries—to double or even triple your absorption. On the flip side, avoid taking iron with calcium supplements, dairy, tea, or coffee, since these all block your ability to absorb iron from food and pills alike.
Next, movement matters. Regular exercise, especially weight-bearing and aerobic activity, helps keep your red blood cell production steady and can even lower chronic inflammation, which in turn helps keep hepcidin in check. But there is a caveat: intense endurance sports, especially distance running, can actually raise hepcidin temporarily, making timing of supplementation important. If you exercise hard, consider taking your iron dose in the evening, when hepcidin naturally dips.
Sleep is another piece. Poor or disrupted sleep increases inflammation, which can raise hepcidin and block absorption. Prioritize seven to nine hours of quality sleep, and address sleep apnea if you snore or wake up unrefreshed.
Chronic low-grade inflammation is the silent saboteur. Obesity, metabolic syndrome, autoimmune diseases, gum disease, and even mild infections can all push hepcidin up, locking away your iron. If your labs are stubborn despite the right iron plan, treating underlying inflammation—with better nutrition, regular movement, and sometimes medical therapy—can make all the difference.
If you are pregnant, postpartum, or have heavy periods, your iron needs are higher, but your absorption is not unlimited. In these situations, stick to the evidence-based protocol, monitor your labs every trimester, and adjust only with guidance. For older adults, absorption may slow, and the risk of excess iron rises, so regular monitoring is even more important.
The bottom line? The right supplement is only part of the puzzle. Your daily choices—what you eat, how you move, and how you manage stress and inflammation—are the real levers that determine if your iron plan works.
Not every dip in energy means low iron, and not every bout of brain fog is a sign you need a supplement. But certain patterns, especially when they persist over weeks to months, should prompt a closer look.
Early signs of iron deficiency often show up before your blood counts drop. You might notice fatigue that does not go away with rest, shortness of breath with normal activity, or trouble focusing at work or school. Some people develop restless legs at night, or start craving ice, clay, or other non-food items—a sign called pica.
Your brain may feel slower, with more difficulty remembering things or a low mood that does not make sense. In women, heavy periods or new onset of heavier bleeding can be a red flag. In men or older adults, new fatigue, pale skin, frequent infections, or unexplained bruising should be taken seriously, especially if you are also losing weight without trying.
If you are taking iron and your symptoms do not improve after two to three months, or if your labs show no change, do not just keep increasing the dose. Ask for a full iron panel, including ferritin, serum iron, TSAT, TIBC, and inflammation markers like CRP or IL-6. Persistent low iron despite supplements can signal hidden blood loss from the gut, chronic inflammation, or, rarely, a genetic absorption problem.
If you develop severe fatigue, chest pain, rapid heart rate, or notice blood in your stool or urine, seek medical care promptly. These can be signs of significant anemia or internal bleeding and need urgent evaluation. And if your ferritin climbs above three hundred, especially with normal or low iron and TSAT, discuss the risk of iron overload or undiagnosed inflammation with your doctor.
In short, listen to your body’s early signals. Track your symptoms, match them to your labs, and do not hesitate to ask for a more complete workup if things are not adding up. The right information can transform frustration into a plan that actually works.
You started this journey thinking more iron might be the answer to fatigue, brain fog, or poor immunity. But now you know—the true gatekeeper is hepcidin, your body’s own traffic director for iron absorption.
High-dose supplements are not always better, and sometimes they do nothing at all if your hepcidin is high. The best results come from matching your supplement dose to what the evidence shows works—about sixty milligrams of elemental iron daily for most people—then monitoring the right numbers: serum iron, transferrin saturation, and ferritin, with inflammation markers to interpret the results.
Addressing lifestyle levers—like eating iron-rich foods with vitamin C, avoiding absorption blockers, exercising regularly, and tackling chronic inflammation—sets the stage for your protocol to work. If your numbers or symptoms do not improve, do not just push harder. Instead, look for the real blockers: inflammation, hidden blood loss, or rare absorption disorders. Sometimes, intravenous iron is the right next step.
Your body is not a black box. It gives you signals—through symptoms, through lab markers, and through how you feel day to day. The smartest approach is to work with your biology, not against it. That means using science, not guesswork, to guide your iron plan. If you act on this knowledge, you can move from frustration to progress, and get back to living with energy, clarity, and resilience. The best time to rethink your iron strategy is before things spiral. The second best time is today.
Why Your Iron Supplement Dose May Not Matter—But Your Hepcidin Level Does
How your body's iron gatekeeper determines whether any dose works at all
Diagram glossary
- CRP:
- A blood test marker used to detect and measure inflammation in the body.
- ferroportin:
- The primary iron exporter protein located in the gut and storage cells.
- IL-6:
- A marker of inflammation that can be tested if iron levels do not rise.
Conclusions
The key lesson is simple. More iron is not always better. Evidence in pregnancy shows ≤60 mg elemental iron daily can work as well as higher doses. Whether you improve may depend more on hepcidin than on dose. If your labs do not move after 8–12 weeks, look for inflammation or ongoing blood loss instead of just taking more pills.
The strongest dose-comparison evidence comes from pregnancy trials, so other groups may differ. Hepcidin tests are not widely available, so many people must infer high hepcidin from inflammation markers and poor response. Serum iron and TSAT can vary by time of day and recent meals, so repeat testing and consistent timing help. This article is educational and does not replace medical care, especially in pregnancy, kidney disease, or suspected bleeding.
Track this in your stack
See how iron relates to your health goals and monitor changes in your biomarkers over time.