
Why Your Vitamin C Levels Predict Bone Loss Better Than Your Age
How Tracking This Overlooked Nutrient Can Help You Protect Your Bones—At Any Stage of Life
Most people think bone loss is inevitable as you age, but new research reveals a surprising fact: your vitamin C level predicts bone mineral density better than your birth year.
In other words, it's not just about getting older—it's about whether your body has enough vitamin C to keep your bones strong. This matters because low bone density means higher risk of fractures, and most people never find out they're vitamin C deficient until damage is done.
Here's what the latest studies show: vitamin C deficiency is common, especially in adults under 50 and postmenopausal women. Low vitamin C predicts bone loss and fracture risk, even when calcium and vitamin D intake are adequate. The connection isn't just theory—it's measurable in your blood. Doctors rarely check vitamin C status, so many people miss the chance to correct a hidden driver of osteoporosis. Addressing this gap can change your bone health trajectory at any age.
If you want to protect your bones, start by tracking your plasma vitamin C. Aim for at least 60 micromoles per liter, with optimal levels above 75. Research suggests taking 500 mg of vitamin C twice daily—preferably as ascorbic acid or a liposomal formulation for best absorption—can boost blood levels and slow bone loss. For most adults, this means a morning and evening dose, ideally with meals and combined with 1,000-2,000 IU of vitamin D3 for added synergy. If you want stronger bones, fewer fractures, and a more predictable way to track your progress, make vitamin C as essential in your routine as calcium or vitamin D.
- Liposomal
- A delivery form that wraps a compound in tiny fat-like spheres to improve absorption or stability.
- Liposomal Vitamin C
- A form of vitamin C surrounded by a fatty layer (liposome) that can improve absorption and raise plasma levels more efficiently than regular forms.
- Bone Mineral Density
- A measurement of how much mineral (mainly calcium) is packed into your bones, used to assess bone strength and fracture risk. Higher density means stronger bones; lower density indicates osteoporosis
- Ascorbic Acid
- The basic, most common chemical form of vitamin C found in supplements and foods. It is the standard form your body absorbs and uses to support bone and tissue health.
- MK-7
- A branded vitamin c product family name used to identify a specific extract or formulation in research and supplement labels.
- Plasma Vitamin C
- The level of vitamin C measured in your blood plasma. This is the most reliable way to check if your body has enough vitamin C for bone protection.
- Enteric-coated
- A dosage form designed to resist stomach acid and release later in the intestine.
- Ascorbate
- An active form of vitamin C essential for collagen synthesis and osteoblast differentiation.
- BMD
- Bone mineral density is a clinical measure of mineral concentration in bone tissue.
- cAMP
- A secondary messenger important in many biological processes and intracellular signal transduction.
- CBFA1
- A master transcription factor, also known as Runx2, that regulates osteoblast differentiation.
- CYP2R1
- An enzyme responsible for the principal 25-hydroxylation of vitamin D in the liver.
You probably hear a lot about calcium and vitamin D for bone health, but vitamin C rarely makes the headlines. Yet, the latest research shows your vitamin C status is a more reliable predictor of bone mineral density than your age, especially if you’re under 50 or postmenopausal.
Why does this matter? Bone loss isn’t just a slow, age-driven process. It’s influenced by nutrients in your blood that control how bones renew, repair, and resist fractures. A 2024 meta-analysis found that people with higher plasma vitamin C had stronger bones—even after adjusting for age, activity, and diet. In fact, when vitamin C was low, bone loss accelerated, regardless of how much calcium or vitamin D was present [4][6][12].
Most doctors don’t routinely check your vitamin C levels, but this marker is easy to measure—and it changes faster than your bone scans do. Standard plasma vitamin C ranges are 23–85 micromoles per liter, but studies show bone protection starts above 60, with optimal effects above 75. Levels below 23 are considered deficient and can lead to a sharp drop in bone strength within months.
Here’s why this matters for you: if your vitamin C is low, your risk of osteoporosis and fractures jumps, sometimes before you ever notice symptoms. Early warning signs—like slow wound healing, gum bleeding, or easy bruising—are often ignored, but in adults under 50, these can be the first clues your bones are at risk. The next section explores how vitamin C acts inside your bones—and why deficiency is so damaging, even if you’re getting enough calcium.
It’s tempting to think of vitamin C as just a collagen co-factor, but its role in your bone health goes much deeper. Sure, collagen forms the framework that holds minerals in your bones, but vitamin C is also a powerful antioxidant and a regulator of bone cell activity.
Recent studies show that vitamin C deficiency disrupts the balance between bone-forming cells (osteoblasts) and bone-resorbing cells (osteoclasts). In animal models, vitamin C deficiency rapidly deteriorates bone microarchitecture—meaning the fine structure inside your bones weakens, making them more likely to fracture [12]. In humans, low plasma vitamin C is linked with higher markers of oxidative stress and inflammation, both of which speed up bone loss [3][6].
Here’s what moves your vitamin C biomarker: dietary intake, absorption efficiency, and oxidative stress load. High stress, smoking, and chronic illness can drain your vitamin C faster, dropping blood levels within weeks. Raising your vitamin C intake—especially through supplements—can boost plasma levels in as little as 2–4 weeks, with bone density improvements measurable within 6–12 months [2][4].
Vitamin C also interacts with other bone markers. For example, low vitamin C amplifies the negative effects of vitamin D deficiency, leading to even steeper drops in bone density [5]. Because it also supports vitamin K recycling and nitric oxide production, vitamin C acts as a keystone nutrient for bone remodeling. Next, we’ll dive into the dose-response relationship and why the amount—and form—of vitamin C you take changes your results.
You might assume that the recommended dietary allowance (RDA) for vitamin C—about 75 mg for women and 90 mg for men—is enough for bone health. But new evidence shows that’s just enough to prevent scurvy, not to optimize bone density. So, what’s the right dose?
A 2022 meta-analysis found that each 100 mg increase in daily vitamin C intake was linked to measurable gains in bone mineral density at the femoral neck and lumbar spine [2][6]. Other cohort studies show women in the lowest tertile for vitamin C intake (7–57 mg/day) lost bone twice as fast as those consuming over 100 mg/day [13]. For clear bone protection, studies suggest at least 500 mg twice daily—a total of 1,000 mg per day—delivered as ascorbic acid or, for those with digestive sensitivity, liposomal vitamin C [2][4][12].
Here’s why form matters: ascorbic acid is well-absorbed at doses up to 500 mg at a time, but absorption drops above this unless you use a liposomal or slow-release formulation. Liposomal vitamin C surrounds the nutrient in a fat bubble, boosting its bioavailability and raising plasma levels more efficiently [key_terms]. Enteric-coated versions can also help if you experience GI upset.
Stacking vitamin C with vitamin D3 (1,000–2,000 IU daily) and vitamin K2 (90–180 mcg, in menaquinone-7 form) creates synergistic effects—each supports the others' bone-building actions [5][3]. If you’re tracking biomarkers, expect plasma vitamin C to rise within 2–4 weeks of supplementation, with bone density changes becoming measurable at 6–12 months. The next section will break down how these effects look in different demographic groups, so you can personalize your approach.
Not all bone loss is created equal. The impact of vitamin C on bone density varies by age, sex, and even underlying health conditions. Let’s explore how different groups respond—and what early warning signs to watch for.
For men under 50, a 2022 study found that suboptimal plasma vitamin C strongly predicted low lumbar spine bone mineral density, even after adjusting for calcium, vitamin D, and activity [4]. In this group, vitamin C deficiency moved the BMD needle more than age or BMI—a finding that flips conventional wisdom. Early warning signs include unexplained muscle weakness, frequent sprains or stress fractures, and slow recovery from exercise.
Postmenopausal women are another high-risk group. Loss of estrogen accelerates bone turnover, and vitamin C deficiency amplifies this effect. A Boston Puerto Rican Health Study found that women with plasma vitamin C below 60 micromoles per liter had significantly lower hip and lumbar spine BMD, regardless of calcium intake [6]. These women also showed higher oxidative stress, which is both a risk factor and an early sign of compromised bone remodeling. Symptoms like bleeding gums, dental issues, or persistent fatigue may be the first hint that your vitamin C status is putting your bones at risk.
People with diabetes or digestive conditions, like short bowel syndrome, also see faster bone loss when plasma vitamin C is low [8][15]. For these groups, monitoring blood vitamin C every 3–6 months and aiming for levels above 75 micromoles per liter is especially important. In the next section, we’ll dig into the timelines—how quickly vitamin C changes show up in your biomarkers and bone structure.
You want results you can measure. So, how soon do vitamin C changes show up in your blood—and your bones?
Plasma vitamin C is responsive to your intake and stress levels. If you increase your supplement dose or switch to a more bioavailable form, plasma levels can rise within 2–4 weeks. This makes it a powerful, trackable biomarker for your intervention. For most adults, aiming for a plasma level above 75 micromoles per liter is optimal for bone health and antioxidant protection [4][6][8].
Bone mineral density, however, changes more slowly. Studies tracking BMD after increasing vitamin C intake show detectable improvements at 6–12 months, with the fastest changes in people who were previously deficient [2][13]. In one prospective cohort, women in the highest vitamin C intake group lost half as much bone per year as those in the lowest group—visible within one year of tracking [13].
Bone microarchitecture, the fine structure inside your bones, can deteriorate within months if vitamin C drops sharply. Animal studies show that vitamin C deficiency can damage bone microarchitecture in as little as 8 weeks, especially in males [12]. Early biomarker changes—such as rising markers of bone turnover (like alkaline phosphatase) or increased oxidative stress—often appear before changes in bone density. That’s why regular testing of both plasma vitamin C and bone markers is valuable if you’re in a high-risk demographic. Next, let’s look at intervention strategies—how to choose the right supplement, dosing schedule, and stacking partners for your situation.
Not all vitamin C supplements work the same way for bone health. The form, dose, and how you combine it with other nutrients can change your results dramatically.
Ascorbic acid is the standard form used in most research and is effective at doses up to 500 mg per serving. Studies show that taking 500 mg twice daily—morning and evening, ideally with food—maintains higher plasma levels throughout the day than a single large dose [2][4]. If you experience digestive upset, consider liposomal vitamin C, which is absorbed more efficiently, or enteric-coated tablets. These forms bypass the stomach and deliver more vitamin C to your bloodstream, raising plasma levels with less GI discomfort [key_terms].
Stacking matters. Vitamin C works synergistically with vitamin D3 (1,000–2,000 IU daily) and vitamin K2 (90–180 mcg, menaquinone-7). A 2024 study found that combined vitamin C and D deficiency nearly doubled the risk of vertebral fractures compared to deficiency in either alone [5]. For bone repair or after injury, adding magnesium (200–400 mg/day) and silicon (10–30 mg/day) can further support bone remodeling. Always track your plasma vitamin C and bone markers when starting a new stack—adjust your dose every 8–12 weeks based on results.
One key study found that multivitamin blends with high vitamin C actually raised liver enzymes in some people, so avoid mega-dosing above 2,000 mg daily unless you’re under medical supervision [23073950]. The next section will explore how to monitor your progress—what labs and early signs to watch for, and how to personalize your approach based on your biomarkers.
Precision matters. Tracking your vitamin C status and bone health is more effective than guessing or waiting for symptoms. Here’s how to do it.
The best biomarker for vitamin C status is plasma vitamin C. Standard labs consider 23–85 micromoles per liter normal, but you’ll want to aim for 60–75 or higher for bone protection. If your level falls below 23, you’re clinically deficient, and bone loss can accelerate within months [4][6]. Test every 3–6 months, especially if you’re changing supplements, increasing dose, or have risk factors (smoking, diabetes, digestive conditions).
For bone, dual-energy X-ray absorptiometry (DEXA) scans provide your BMD at the hip and spine. Track your T-score and Z-score annually if you’re at risk. Alkaline phosphatase and osteocalcin are blood markers that reflect bone turnover—rising levels may indicate increased bone breakdown, especially if paired with low vitamin C.
Early warning signs of deficiency include slow wound healing, bleeding gums, easy bruising, muscle weakness, or recurring fractures. In younger men, stress fractures or slow recovery from sports may be the first clue. For postmenopausal women, dental issues and sudden changes in grip strength are worth noting. If you see these, check your plasma vitamin C and adjust your supplement regimen accordingly.
Personalize your approach. If your vitamin C is optimal and you’re still losing bone, look at stacking with D3, K2, or magnesium, and address any absorption or digestive issues. In the final two sections, we’ll review the research limitations and summarize what you need to remember for lifelong bone strength.
Emerging research shows that vitamin C’s role in bone health is not one-size-fits-all. The effects vary by sex, age, and even hormonal status—making it critical to tailor your approach.
In men under 50, a recent cross-sectional study found that suboptimal vitamin C was a stronger predictor of low lumbar spine BMD than either age or BMI [4]. This means that men who ignore their vitamin C status, even if they’re young and active, can be at higher risk for early bone loss. Early intervention—raising plasma vitamin C above 75 micromoles per liter—produced the biggest gains in BMD in this group, especially when paired with vitamin D3 and resistance exercise.
In postmenopausal women, estrogen loss accelerates bone turnover. Studies show that vitamin C deficiency magnifies this effect, leading to faster bone loss and higher fracture risk [6][10][13]. In these women, even small increases in vitamin C intake (from 75 to 500 mg/day) slowed bone loss by 30–50% over one year. Combining vitamin C with vitamin K2 and D3 provided the most robust protection.
Animal research provides further nuance. One study found that vitamin C deficiency deteriorates bone microarchitecture more severely in adult male mice than in females, suggesting hormonal status and sex hormones may modulate the impact [12]. For both sexes, the interplay between vitamin C, vitamin D, and oxidative stress is key—deficiencies in more than one nutrient compound the risk. Next, we’ll close with practical takeaways and how to apply this knowledge to your supplement routine for maximum bone protection.
Vitamin C is more than a generic antioxidant—it’s a trackable biomarker and a critical driver of bone mineral density at every age. Here’s how to leverage the latest evidence for your bone health:
First, test your plasma vitamin C. Don’t rely on diet guesses or symptoms alone. Target a level above 60 micromoles per liter, with optimal protection above 75. If you’re under 50, postmenopausal, diabetic, or have gut issues, check every 3–6 months.
Second, supplement smartly. Aim for 500 mg of ascorbic acid or liposomal vitamin C twice daily, with meals, for best absorption and stable blood levels. Stack with 1,000–2,000 IU of vitamin D3 and 90–180 mcg of vitamin K2 (MK-7), adjusting based on your labs and risk factors. If you notice GI discomfort, switch to a liposomal or enteric-coated form.
Third, monitor your progress. Get DEXA scans yearly if you’re at risk, and watch for early warning signs—bruising, bleeding gums, muscle weakness, or stress fractures. Adjust your dose and stack as needed, and remember that changes in bone density take months, but plasma vitamin C responds in weeks.
Vitamin C is the missing link in most bone health strategies. Treat it as essential as calcium or vitamin D, and you’ll have a measurable, actionable way to protect your bones for life.
Why Your Vitamin C Levels Predict Bone Loss Better Than Your Age
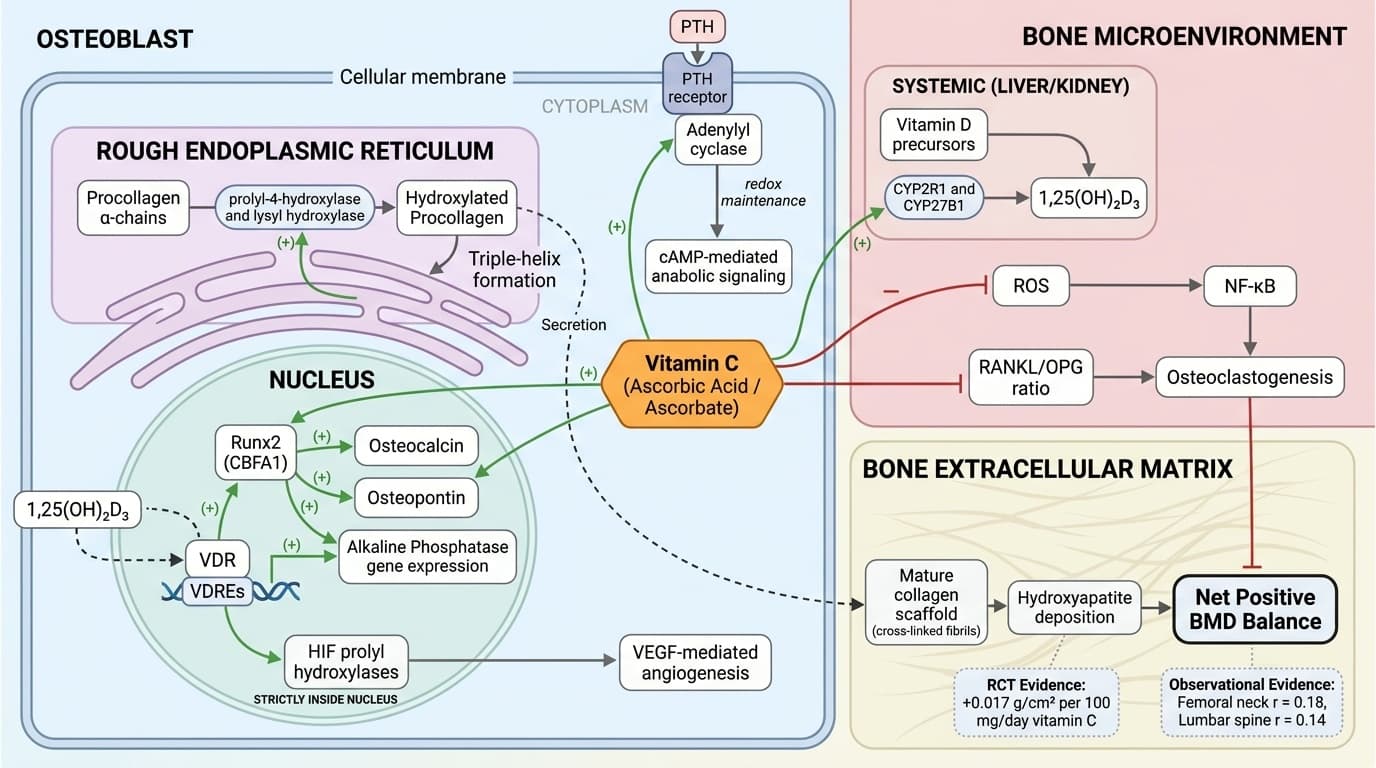
Schematic of vitamin C (ascorbic acid) mechanisms regulating bone mineral density, organized across three compartments: the osteoblast endoplasmic reticulum/nucleus, the bone extracellular matrix, and the bone microenvironment. In the endoplasmic reticulum, ascorbate activates prolyl-4-hydroxylase and lysyl hydroxylase (activation arrows) to hydroxylate procollagen, enabling triple-helix formation and secretion of mature collagen scaffold; in the nucleus, ascorbate promotes Runx2 and osteocalcin gene expression (activation arrows) while vitamin D/VDR signaling provides a feed-forward amplification loop. In the extracellular matrix compartment, properly cross-linked collagen fibrils serve as nucleation sites for hydroxyapatite deposition, with the dose-dependent BMD gain of +0.017 g/cm² per 100 mg vitamin C annotated at this node. In the bone microenvironment, inhibition arrows depict ascorbate's suppression of ROS→NF-κB→osteoclastogenesis and reduction of the RANKL/OPG ratio, while a separate activation arrow shows ascorbate supporting CYP27B1-mediated 1,25(OH)₂D₃ synthesis, which feeds back to osteoblast differentiation; pooled correlation coefficients (femoral neck r=0.18, lumbar spine r=0.14) are annotated on the net BMD output node to anchor the diagram in clinical evidence.
Diagram glossary
- Ascorbate:
- An active form of vitamin C essential for collagen synthesis and osteoblast differentiation.
- BMD:
- Bone mineral density is a clinical measure of mineral concentration in bone tissue.
- cAMP:
- A secondary messenger important in many biological processes and intracellular signal transduction.
- CBFA1:
- A master transcription factor, also known as Runx2, that regulates osteoblast differentiation.
- CYP2R1:
- An enzyme responsible for the principal 25-hydroxylation of vitamin D in the liver.
- D/VDR:
- The signaling complex formed when vitamin D binds to its specific nuclear receptor.
- HIF:
- Hypoxia-inducible factor is a transcription factor that responds to changes in cellular oxygen levels.
- PTH:
- Parathyroid hormone regulates serum calcium concentration through its effects on bone and kidneys.
- RANKL/OPG:
- A signaling axis that regulates bone resorption by controlling osteoclast differentiation and activity.
- ROS:
- Reactive oxygen species are highly reactive oxygen-containing molecules that can cause cellular damage.
- VDRE:
- A specific DNA sequence that binds the vitamin D receptor to regulate gene transcription.
- VEGF:
- Vascular endothelial growth factor is a signaling protein that stimulates new blood vessel formation.
Conclusions
Vitamin C is a powerful and often overlooked driver of bone mineral density—sometimes even more predictive of bone loss than age itself. By tracking plasma vitamin C and using targeted supplementation, you can slow or even reverse bone loss, regardless of your age or sex. The best results come from using bioavailable forms, stacking with vitamin D3 and K2, and personalizing your approach based on biomarkers and risk factors. Making vitamin C a core part of your bone health routine gives you a precision tool to protect your skeletal strength for decades to come.
While the evidence linking vitamin C status to bone mineral density is robust, most studies to date are observational or cross-sectional, with fewer long-term randomized trials. Dose-response effects are better established for adults than for children or teens. There is limited data on optimal upper limits for supplementation in people with kidney issues or rare metabolic disorders. Biomarker ranges can vary by lab and population, and not all studies control for all possible confounders (like unmeasured dietary factors or genetic differences in absorption). Finally, while animal studies show rapid changes in bone microarchitecture with vitamin C deficiency, more research is needed to confirm these effects and timelines in diverse human populations.
Track this in your stack
See how vitamin c relates to your health goals and monitor changes in your biomarkers over time.