
Your B12 Supplement May Be Doing Nothing — Unless You Know Your Absorption Type
Why the right test (and delivery method) matters more than the dose on the label
You might pop a B12 supplement with your morning coffee and assume the job is done.
But the truth is, whether that pill helps your body or simply passes through depends on the invisible details of your own biology. Today, you’ll learn why B12 is the most misunderstood vitamin for gut health, which tests actually reveal if you’re reaping the benefits, and what practical steps you can take to ensure your energy and nerves are truly protected.
- Intramuscular (IM) Injection
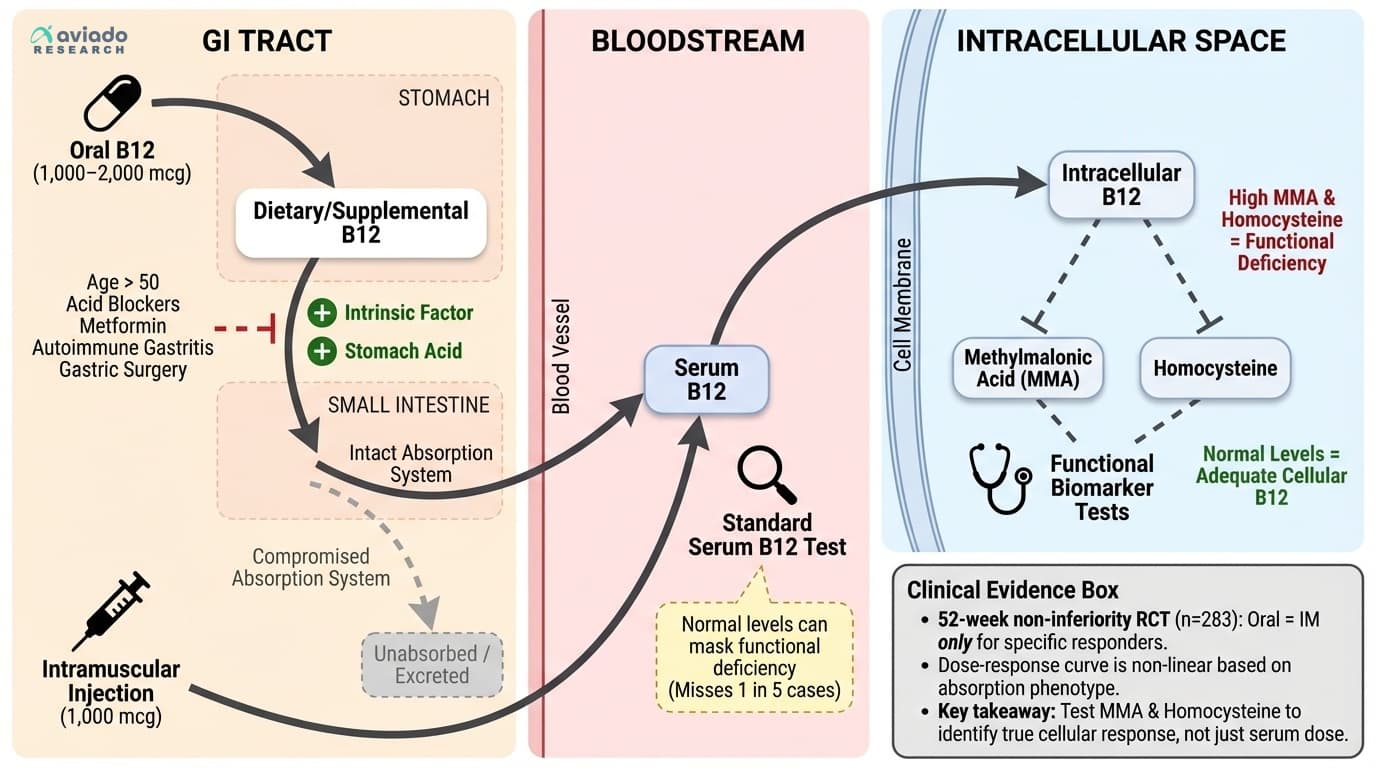
- Delivering medication directly into a muscle. For B12, IM injections bypass the gut and are used when absorption is a problem.
- Methylmalonic Acid (MMA)
- A substance in the blood that builds up when B12 isn't working properly inside your cells. High MMA means you're functionally B12 deficient, even if your blood B12 looks normal.
- Serum B12
- A blood test measuring total B12 in your bloodstream. Can miss functional deficiencies where B12 isn't reaching cells despite normal blood levels.
- Intrinsic factor
- A protein made in the stomach that binds to vitamin B12 and allows it to be absorbed in the small intestine. Without enough intrinsic factor, your body cannot properly absorb B12, even if you consume
- Homocysteine
- Homocysteine, an amino acid metabolite influenced by B vitamins. elevated levels damage blood vessels and increase cardiovascular and dementia risk.
- Absorption Type
- Whether your body can properly absorb B12 from oral supplements. "Responders" absorb well; "non-responders" need injections due to digestive issues or genetic factors.
- Methylcobalamin
- A bioactive form of vitamin B12 that some supplements use. It is already in a form the body can use directly.
- B12
- An essential vitamin whose absorption depends on stomach acid and intrinsic factor.
- g/dL
- A standard unit of measurement representing grams per deciliter, commonly used in blood tests.
- intestine
- The portion of the digestive tract where vitamin B12 is absorbed into the body.
Picture this: you’re standing in your kitchen, vitamins lined up next to the coffee maker. You take your daily B12, confident you’re covering your bases for energy and brain health. But here’s the twist—your friend or partner could take the exact same supplement and feel a surge in energy, while you notice nothing at all.
This isn’t about willpower or placebo. It comes down to something happening deep inside your digestive tract, entirely out of sight. As you swallow that pill, it begins a journey that is far more complicated than most other vitamins. B12 has to navigate stomach acid, bind to a special protein called intrinsic factor, dodge digestive enzymes, and then finally get absorbed in the last part of your small intestine. Any hiccup along this path—maybe a medication you take, a subtle genetic quirk, or changes in your stomach as you age—can mean that B12 never actually makes it into your cells.
And here’s the real kicker: you can have a kitchen drawer full of high-dose B12 tablets, or even a blood test showing plenty of B12 floating in your bloodstream, but still feel tired, foggy, or numb. That’s because the real story is happening at the cellular level, where B12 either sparks your metabolism—or leaves your nerves and energy pathways lagging behind. So how does B12 really work once you swallow it? That’s where the science starts to matter for your daily life.
You might wonder why B12 gets so much attention when it comes to gut health. The answer is in the details of how your body tries to pull this vitamin from food or supplements and get it where it’s needed most: your brain, your nerves, and every cell that needs to make energy.
B12 is unique among vitamins. It’s the largest and most structurally complex, and your body cannot make it on its own. The only natural sources are animal foods or certain bacteria. When you eat or supplement B12, it enters your stomach, where it first binds to proteins. Stomach acid and a digestive enzyme called pepsin are needed to release B12 from food. Then, a special protein called intrinsic factor (made by cells in your stomach lining) grabs on to it. This B12-intrinsic factor complex travels down to the small intestine, where it’s finally absorbed.
Here’s where things get tricky. If your stomach acid is low—which becomes more common as you get older, or if you take acid-blocking medications—B12 doesn’t get released from food. If your stomach lining is damaged, perhaps from autoimmune issues or chronic inflammation, you may not produce enough intrinsic factor. And if you’ve had stomach or intestinal surgery, the whole chain can break down.
Your genetics play a role as well. Some people have gene variations that affect intrinsic factor, or the cell receptors that absorb B12, making them 'non-responders' to oral supplements. Others absorb B12 efficiently, no matter what form it’s in.
This is why B12 deficiency is especially common after age fifty, in vegetarians or vegans, in people with digestive disorders like celiac or Crohn’s disease, and in anyone taking medications like metformin or proton pump inhibitors for heartburn. But even if you don’t fit any of these categories, subtle absorption issues can still sneak up on you. The bottom line: your gut health and your unique biology are the gatekeepers for whether that B12 supplement ever goes to work in your cells. The difference can shape your energy, mood, memory, and nerve health for years to come.
So how do you actually know where you stand with B12? That brings us to the biomarkers that matter most.
When you go to your doctor and ask about your B12 status, the answer usually comes back in the form of a serum B12 blood test. But here’s the hard truth: this test only shows how much B12 is floating around in your bloodstream at the moment, not what’s making it into your cells and doing the real work.
What matters is functional sufficiency—whether B12 is reaching your tissues and powering metabolism. This is where two overlooked markers come into play: methylmalonic acid, or MMA, and homocysteine. When your cells are starved for B12, MMA and homocysteine start to build up. MMA rises because B12 is needed to help break it down. Homocysteine goes up when B12-driven reactions stall, putting strain on your cardiovascular system and raising risk for nerve damage and cognitive decline.
A growing body of research, including a review published in the American Journal of Clinical Nutrition, shows that up to one in five people with 'normal' B12 blood levels still have signs of functional deficiency. That means their cells are not getting the B12 they need, and symptoms like fatigue, numbness, memory problems, and even mood changes are much more likely. If you’re relying on a serum B12 test alone, you could easily miss a hidden deficiency—the kind that does real damage over time.
Here’s how to interpret these markers for your own health. For methylmalonic acid, you’ll want to see levels below two hundred sixty nanomoles per liter. Higher numbers suggest your cells can’t process B12 properly. For homocysteine, most labs consider anything below ten micromoles per liter as safe, but the optimal range is closer to six to eight. If either marker is elevated, it’s a red flag that your B12 supplement—or dietary intake—isn’t doing its job where it counts.
Why does this matter? Because correcting functional B12 deficiency—not just boosting blood levels—has been linked to improvements in memory, energy, and nerve function. In fact, trials show that bringing MMA and homocysteine down into the optimal range can reverse symptoms that traditional tests would have missed. This puts the power to truly measure and track your B12 health in your hands, not just on a lab slip.
Let’s get practical. If you’re looking to optimize your B12—and actually feel the benefits—your approach should match your unique absorption profile. Here’s how to tailor your protocol so you’re not just guessing.
For people with healthy stomachs and no known absorption issues, research shows that one thousand to two thousand micrograms of oral B12 daily is typically effective. Studies, including a large review from the British Journal of Haematology, found that these doses can reliably restore B12 status for most healthy adults, even those on plant-based diets. The reason for the high dose? Only a tiny fraction is absorbed by passive diffusion, so you need more in the pill than your body actually keeps.
But if you’re over fifty, have digestive disorders, or take medications like metformin or acid blockers, you might fall into the 'non-absorber' category. For you, swallowing more and more B12 often does nothing. A landmark Finnish trial in 2024 followed over two thousand older adults and found that those with low intrinsic factor or prior gastric surgery needed a completely different approach: monthly intramuscular injections of one thousand micrograms. This bypasses all the gut bottlenecks and ensures B12 reaches your bloodstream and cells directly.
There is also growing evidence for high-dose sublingual B12—tablets that dissolve under your tongue—especially for people who cannot tolerate injections. These forms are absorbed directly through the mucous membranes, offering a workaround for some absorption barriers.
The key is to test your MMA and homocysteine before you start any new protocol. Take your chosen form—oral, sublingual, or injection—then retest after twelve weeks. If your markers normalize, you’ve found what works for you. If not, it’s time to change approach. This personalized method, grounded in your own biology, is the difference between a supplement that collects dust and one that actually transforms your energy and nerve health.
What about plant-based sources? That’s the next piece of the puzzle.
If you follow a vegetarian or vegan diet, you’ve likely heard the warning: plant foods don’t provide real B12. For decades, nutritionists believed that only animal products contained the active, absorbable form. But recent research challenges this old wisdom and opens new options for those avoiding meat and dairy.
A clinical trial published in Nutrition Research in 2021 put plant-derived B12 to the test. Researchers gave vegetarian adults nori—a type of edible seaweed common in sushi—along with measured amounts of B12-fortified foods. The results were striking. Not only did B12 from nori raise blood levels, but it also improved MMA and homocysteine, the true markers of cellular B12 sufficiency. The effect was dose-dependent: the more nori consumed, the greater the impact on B12 status. This means that certain plant-based sources, when chosen carefully, can actually deliver bioactive B12.
However, not all plant-based B12 is created equal. Some forms found in algae and fermented foods are inactive analogs—they look like B12 but do not work in your body. Only specific sources, like nori and some fortified nutritional yeasts, have been shown to move the needle on functional markers. The mechanism here is simple. Nori contains methylcobalamin and adenosylcobalamin, two active forms of B12, which your body recognizes and uses just like the B12 from animal foods or supplements.
If you’re plant-based, aim for at least two to three servings of nori per week, or use a B12-fortified food with at least one hundred micrograms per serving. Still, it remains wise to check your MMA and homocysteine regularly, as absorption can vary. For most people, supplementing with oral B12—cyanocobalamin or methylcobalamin—is the most reliable way to ensure sufficiency, regardless of diet. The bottom line: the right plant-based sources can contribute to B12 status, but testing and targeted supplementation remain essential to avoid silent deficiency.
So you know what to take and what to look for in your labs. But your daily habits and medications can make or break your B12 strategy. That’s what we’ll cover next.
Supplements are only one piece of the puzzle. Your everyday choices—what you eat, how you manage stress, what medications you take—all influence whether B12 reaches your cells and does its job.
Start with your gut health. Chronic inflammation in your stomach, often from Helicobacter pylori infection, autoimmune gastritis, or years of acid-suppressing medications, can limit the production of intrinsic factor. Without this protein, even the best diet or supplement can’t deliver B12 where it’s needed. If you have a history of reflux, ulcers, or digestive issues, it’s worth discussing with your doctor whether you might be at risk for low stomach acid or intrinsic factor.
Diet matters, too. Animal foods—especially shellfish, liver, beef, eggs, and dairy—are naturally rich in B12. If you eat these regularly, your risk of deficiency is lower, but absorption still depends on gut health. For those on plant-based diets, as we discussed earlier, fortified foods and careful supplementation are essential.
Medications are a major overlooked factor. Proton pump inhibitors like omeprazole, H2 blockers like ranitidine, and the diabetes drug metformin are all known to reduce B12 absorption. A large meta-analysis published in JAMA in 2020 found that people on long-term acid blockers had a significantly higher rate of B12 deficiency, especially after two or more years of use. If you’re on these medications, check your functional B12 markers at least once a year, and consider switching to injections or sublingual forms if your levels are borderline.
Even your stress level plays a role. Chronic stress can alter stomach acid production and gut motility, both of which can influence B12 absorption. Mindful eating, stress-reduction practices, and avoiding unnecessary medications all help protect your gut’s ability to process B12.
Physical activity is another positive lever. Regular exercise has been shown to improve gut motility and overall digestive health, which may indirectly support nutrient absorption. The takeaway: your supplement is only as effective as the environment you give it. Treat your gut well, review your meds, and keep lifestyle factors working for—not against—your B12 strategy.
Now, how do you know if something is going wrong before major symptoms appear? Let’s talk about early warning signs.
You might not notice B12 deficiency right away. The symptoms are subtle at first, but over time, they add up—and can become serious if ignored. Recognizing these early warning signs allows you to act before real damage is done.
Fatigue is usually the first clue. If you feel unusually tired despite getting enough sleep, or your energy crashes in the afternoon, your cells may not be making energy efficiently due to low B12. This is especially true if you’ve recently changed your diet, started new medications, or have digestive issues.
Nerve symptoms are another red flag. Tingling, numbness, or a 'pins-and-needles' feeling in your hands or feet can be the earliest hint that your nervous system is struggling without enough B12. Left unchecked, these symptoms can progress to balance problems, memory lapses, or even mood changes like depression and irritability.
Digestive changes can also signal trouble. Loss of appetite, diarrhea, or unexplained weight loss may point to underlying issues with stomach acid, intrinsic factor, or gut health that affect B12 absorption. Even a sore or swollen tongue is a classic but often overlooked symptom.
In older adults, B12 deficiency can mimic dementia, with memory loss and confusion that sometimes reverses when levels are corrected. For younger people, the warning signs are often more about energy, mood, and nerve health.
If you notice any of these symptoms—especially if you have risk factors like a plant-based diet, digestive issues, or use of acid-blockers—don’t wait for things to get worse. Ask your doctor about testing methylmalonic acid and homocysteine in addition to standard B12. Early action can mean faster recovery and prevention of long-term complications.
So what should you do next? Let’s wrap up with a clear path forward.
You’ve learned that B12 is more than just another supplement. It’s a vitamin with a uniquely complex absorption process, shaped by your gut health, genetics, and daily choices. Whether your supplement works depends on factors most people never consider—stomach acid, intrinsic factor, medications, and even the foods you eat.
The standard blood test for B12 is only the beginning. To truly know if you’re getting the benefits, you need to track methylmalonic acid and homocysteine—the functional markers that show whether B12 is actually working inside your cells. For most adults, one thousand to two thousand micrograms of oral B12 daily is effective. But if you’re over fifty, have gut issues, or take medications that block absorption, you may need monthly injections or high-dose sublingual forms to see real improvement.
Plant-based diets can support B12 health, especially with careful use of nori and fortified foods, but testing remains essential to avoid silent deficiency. Your medications, gut health practices, and even your stress level all play roles in how much B12 you actually use. Watch for early symptoms—fatigue, nerve tingling, cognitive changes—and test before symptoms become severe.
The good news is, you have the tools to personalize your B12 strategy and track your progress. Test your markers, tailor your supplement form and dose, revisit your medications with your doctor, and support your gut with healthy habits. With these steps, you can make sure your B12 supplement is actually doing something—and protect your energy, nerves, and brain for years to come.
Your B12 Supplement May Be Doing Nothing — Unless You Know Your Absorption Type
Why the right test (and delivery method) matters more than the dose on the label
Diagram glossary
- B12:
- An essential vitamin whose absorption depends on stomach acid and intrinsic factor.
- g/dL:
- A standard unit of measurement representing grams per deciliter, commonly used in blood tests.
- homocysteine:
- A blood biomarker that rises when vitamin B12 is not functioning properly inside cells.
- intestine:
- The portion of the digestive tract where vitamin B12 is absorbed into the body.
- MMA:
- Methylmalonic acid is a cellular biomarker used to detect hidden vitamin B12 deficiencies.
Conclusions
Vitamin B12 supplementation isn't one-size-fits-all. The latest research makes it clear: your absorption type determines whether oral supplements, injections, or even food sources will work for you. Standard blood tests miss functional deficiencies in 15-20% of cases, so testing MMA and homocysteine is essential to know if B12 is truly working in your body. For those with normal absorption, a daily oral dose of 1,000–2,000 micrograms is usually effective. For non-absorbers, monthly injections of 1,000 micrograms are needed. Test the right markers, know your absorption type, and choose the delivery method that matches your biology.
Most studies on B12 absorption and outcomes use short- to medium-term follow-ups and may not capture long-term neurological effects. Not all research stratifies by absorption phenotype, so individual responses can be hidden in the averages. The availability and insurance coverage of functional tests (MMA, homocysteine) may limit access for some patients. Lastly, while recent data supports nori as a plant-based B12 source, more studies are needed to confirm these findings across different populations.
Track this in your stack
See how vitamin b12 relates to your health goals and monitor changes in your biomarkers over time.
Sources (10)
This article informs how supplementation moves 1 marker.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.