
Your HbA1c Number May Be Lying to You — And Genetics Explains Why
Up to 40% of people have systematic differences between their HbA1c and actual glucose exposure
You might assume your HbA1c test gives you a clear picture of your blood sugar control, but the truth is more complicated.
Your genetics and the biology of your red blood cells can distort this number, meaning your health story might not match what the lab report says. Let’s unravel why HbA1c sometimes lies, what you can do about it, and how to get the most accurate understanding of your metabolic health.
- Time-in-range (TIR)
- The percent of time your CGM glucose stays in a target band, often 70–180 mg/dL.
- Continuous glucose monitor (CGM)
- A wearable sensor that tracks glucose all day and night and shows patterns HbA1c cannot show.
- Hemoglobin A1c
- Average blood sugar over the past 2-3 months by assessing glycated hemoglobin. each 1% increase raises cardiovascular risk by 18%.
- Glucose
- Blood sugar level, the primary energy source for cells. Fasting glucose is normal, prediabetes, ≥126 suggests diabetes.
- Fructosamine
- A blood test that reflects average glucose over about 2–3 weeks by measuring glycated serum proteins.
- HbA1c (hemoglobin A1c)
- A lab test that estimates average glucose by measuring how much glucose sticks to hemoglobin in red blood cells.
- Albumin
- Albumin, the main protein produced by the liver. low levels indicate liver disease, malnutrition, or protein loss.
- CGM
- A wearable device that continuously monitors blood sugar levels throughout the day.
- DNA
- The genetic material that can contain variants affecting red blood cell biology and HbA1c.
- eAG
- Estimated average glucose, a metric translating HbA1c into an average blood sugar level.
Imagine getting your blood drawn after months of careful eating and exercise. You expect a pat on the back, but your doctor frowns at your latest HbA1c result. Or maybe you slip up a little, but your number comes back better than expected. It feels confusing, even unfair. You are not alone. Many people have had the same experience—wondering if their hard work is showing up in their lab results or if something else is going on behind the scenes.
Most of us want our health numbers to reflect our real efforts and risks. But sometimes, the numbers do not add up. You might feel fine, keep your blood sugar meter in check, and still get a high HbA1c. Or you might see a low HbA1c while your daily readings tell a different story. The mismatch can leave you second-guessing your routines, your doctor, or even your own body.
Here is the human truth: your HbA1c is not always a perfect mirror of your average blood sugar. It is shaped by more than just what you eat and how much you move. The test is rooted in biology that can vary from person to person, driven in part by your genetics. That means you could be working with a measuring stick that bends, depending on who you are. Let’s explore why this happens, what it means for your health decisions, and how you can work around the blind spots.
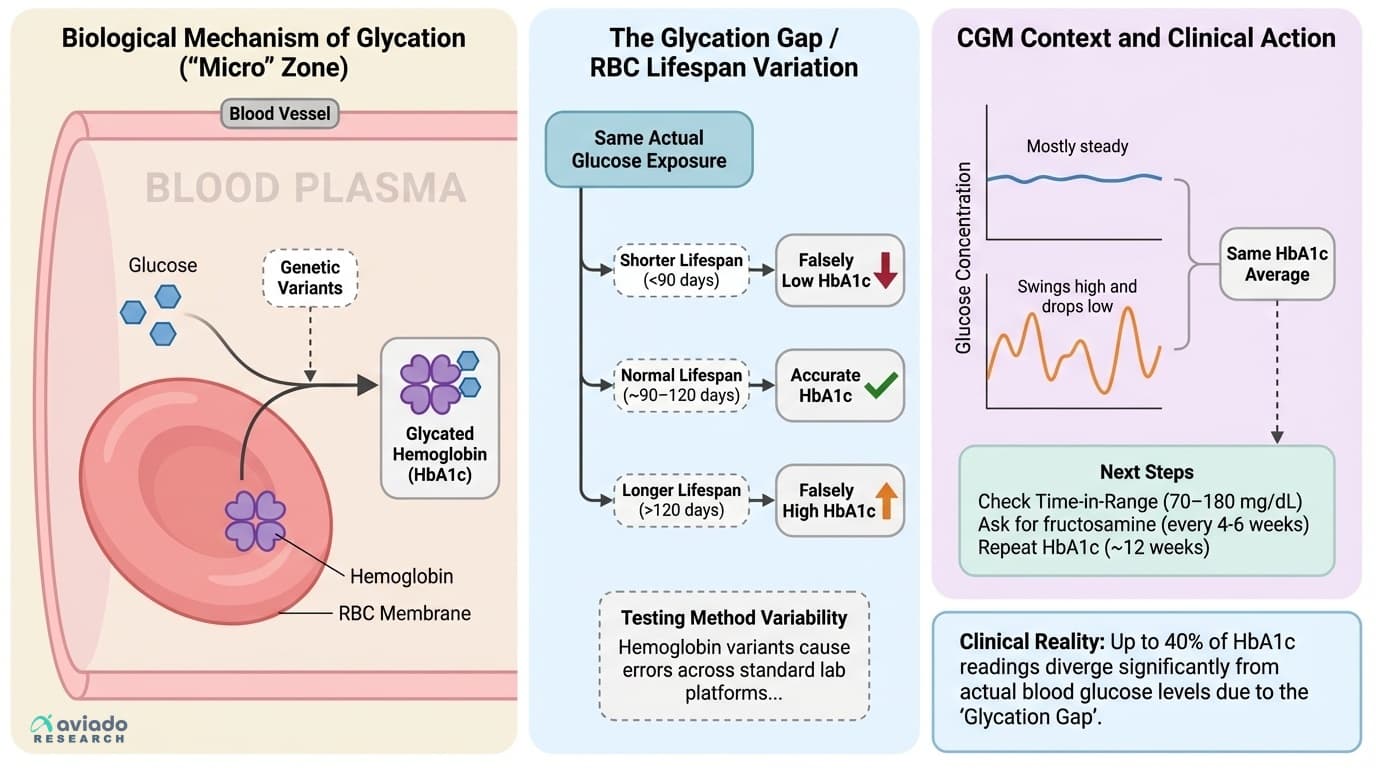
To understand why your HbA1c might not match your lived experience, you need to know how the test works. HbA1c is a measure of how much glucose, or sugar, has attached itself to your hemoglobin—the protein inside your red blood cells that carries oxygen. The more sugar in your blood, the more it sticks to hemoglobin. Doctors and labs use this as a rough average of your blood sugar over the last three months.
But here is the twist. The test assumes your red blood cells live about three to four months—roughly ninety to one hundred twenty days. In reality, that lifespan can swing widely from person to person. Your red blood cells might last two months, or they might stick around for one hundred forty days. This matters because if your red blood cells die off quickly, they have less time to accumulate sugar. Your HbA1c reads lower, even if your average blood sugar is not actually better. On the flip side, if your red blood cells live longer than average, more sugar can attach, and your HbA1c creeps higher—even if your real glucose is well managed.
Genetics come into play as well. Large genetic studies have found that certain DNA variants can change your HbA1c by affecting how your red blood cells are made, how quickly they break down, or even the structure of your hemoglobin itself. One person might consistently run a little higher or lower on HbA1c than someone else with the same blood sugar, simply due to their genes. This effect is not a rare glitch—it is surprisingly common.
Researchers call this stable difference the 'glycation gap.' If your HbA1c always runs high or low compared to your other blood sugar readings, that gap likely will not disappear on its own. It is not about good days or bad days at the lab. It is a sign that your biology is influencing the test as much as your behavior. Understanding this gap is crucial because it can affect your risk assessment and treatment decisions. If you do not recognize it, you might be labeled as high risk or low risk for diabetes and its complications, even when your actual glucose exposure tells a different story.
So, if your doctor ever seems puzzled by your numbers, or if you notice a consistent mismatch between your daily readings and your HbA1c, you are not imagining things. Your biology really can tilt the numbers.
You might think of a lab test as a solid fact, like your height or your birthday. But with HbA1c, the method used can shift your results. This is especially true if you belong to a group with certain hemoglobin variants, which are more common in some populations. For example, people with African, Mediterranean, or Southeast Asian ancestry are more likely to carry these changes in hemoglobin.
Let’s take the case of hemoglobin N Baltimore. This variant can throw off HbA1c measurements dramatically, depending on which testing platform your lab uses. In one comparison across six common methods, some tests gave readings that were too low, while others stayed accurate. That means two people could walk into two different clinics and come out with very different results from the same blood sample. If your results are close to the cutoffs for diagnosing diabetes or prediabetes, this can change your diagnosis, your treatment plan, and even your insurance premiums.
Now, consider point-of-care testing—the kind done right in your doctor’s office with a fingerstick and a small machine. These devices are faster and more convenient, but they are not always as consistent as the big lab machines. Several studies have found that point-of-care HbA1c tests can differ enough from lab-based tests to cause confusion, especially when your result is hovering near a clinical threshold. The type of test your provider chooses—whether it uses ion-exchange chromatography, immunoassay, or enzymatic methods—can all influence your number.
Even as labs work to standardize HbA1c testing, small differences between machines persist. The same blood can give you different answers, depending on how and where it is measured. This is not just a technicality. If your number is right at the edge of a diagnosis, you could be told you have diabetes in one clinic and not in another. This is why it is important to track your results over time, always ask which method is being used, and consider repeat testing or alternative markers if your numbers do not seem to match your experience.
The bottom line here is that HbA1c is not a perfect number. It is an estimate, shaped by your biology and by the tools used to measure it. If something does not add up, you are right to dig deeper. Next, let’s see what continuous glucose monitoring can reveal that HbA1c misses.
Think about what it would feel like to see a movie of your blood sugar, not just a single snapshot. That is what continuous glucose monitoring, or CGM, can do for you. Instead of one average number every three months, you get a running picture—minute by minute, day by day—of how your glucose rises and falls.
Here is why this matters. Two people can both have an HbA1c of, say, six percent. But their daily lives might look totally different. One person’s blood sugar could drift gently up and down within a safe range all day. Another person might spike high after every meal and crash low overnight. The HbA1c does not see those swings. It only sees the average. But those swings matter for your risk of nerve damage, eye disease, and other complications. The bigger your swings, the more stress on your blood vessels and nerves, even if your average looks okay.
CGM adds context. It shows you your time-in-range—the percentage of your day when your glucose is between seventy and one hundred eighty milligrams per deciliter, which is the sweet spot for most people. Experts recommend aiming for at least seventy percent time-in-range for optimal metabolic health. CGM also shows you how much time you spend above or below that zone. That information helps you identify what foods, activities, or stressors push your numbers out of range.
Here is how you can use this data. Compare your CGM average glucose with the estimated average glucose from your HbA1c. If these two numbers differ by more than fifteen milligrams per deciliter, that is a big clue that your HbA1c might not be telling your full story. Maybe your red blood cell biology is skewing the number. Or maybe there is an issue with your testing method. Either way, you deserve to know what’s really happening in your body.
CGM can also help you fine-tune your choices in real time. You can see how a certain breakfast bumps your sugar, or how a walk after dinner brings it down. You are not left guessing. If you do not have access to a CGM, you can still use a fingerstick meter to log before and after meals, but CGM provides a richer, more complete picture.
So, if you are striving for fewer complications and better metabolic health, combine both tools. Use HbA1c for the long view and CGM for the daily details. If they do not match, it is time to look for answers beyond a single number.
When your HbA1c and your real-life glucose readings do not line up, it is time to bring in backup. Two alternative blood tests—fructosamine and glycated albumin—can fill in the gaps. These markers give you a snapshot of your recent blood sugar control, but they are not affected by red blood cell lifespan. That makes them especially helpful if you have a known hemoglobin variant, anemia, kidney disease, recent blood loss, or anything else that might throw off your HbA1c.
Fructosamine measures the amount of glucose attached to blood proteins, mostly albumin, over the past two to three weeks. Because albumin turns over much faster than red blood cells, fructosamine updates more quickly. Most labs report a normal range below two hundred eighty-five micromoles per liter, but your target might depend on your age, health status, and risk factors. Higher values mean higher average glucose over the past few weeks. If you are making rapid changes to your diet, exercise, or medications, fructosamine can reveal whether those changes are working. It is especially useful during pregnancy, after a medication change, or if you are troubleshooting unexplained HbA1c results.
Glycated albumin is similar, but it focuses only on the glucose attached to albumin, with a window of about one to two weeks. This test is less commonly used in the United States but is gaining traction worldwide. It is particularly valuable if you have conditions that change your albumin levels or if you need a very short-term view of your glucose control.
When should you use these tests? If your HbA1c and your CGM or fingerstick numbers disagree by more than fifteen milligrams per deciliter, ask your doctor for a fructosamine or glycated albumin test. If these alternative markers agree with your meter or CGM, you can be more confident in your day-to-day numbers and less worried about a misleading HbA1c. If all three tell a different story, work with your provider to identify whether anemia, kidney disease, or another condition is at play.
The key takeaway is that you are not stuck with just one number. You have options. Using alternative markers helps you personalize your metabolic monitoring, avoid unnecessary worry or overtreatment, and make more informed choices about your health.
Now that you know HbA1c can be misleading, how can you get the clearest possible picture of your metabolic health? The answer is to use a combination of tools—and to know when to dig deeper if the numbers do not make sense. Here is an evidence-based protocol you can follow, whether you are managing diabetes, working on prevention, or just optimizing your health.
First, monitor your blood sugar using a CGM if you can access one. Aim for at least seventy percent of your time in the seventy to one hundred eighty milligrams per deciliter range. If you do not have a CGM, use a meter to check before and after meals and keep a daily log. Look for patterns—what foods or activities push you out of range, and what helps you stay steady.
Second, cross-check your HbA1c with your average glucose from CGM or your logbook. If the estimated average glucose from HbA1c is more than fifteen milligrams per deciliter different from your actual average, flag it. That is your cue to ask about red blood cell lifespan, hemoglobin variants, or lab method issues.
Third, request alternative markers if something seems off. Ask for a fructosamine test every four to six weeks during periods of change, such as after starting a new medication, changing your diet, or recovering from illness. Repeat your HbA1c about every twelve weeks. Use glycated albumin if fructosamine is not available or if you need a very short-term view.
Fourth, track your time-in-range, not just your averages. The more time you spend in the healthy zone, the lower your risk of complications—even if your average looks good on paper. Time-in-range is emerging as one of the most meaningful predictors of long-term health.
Fifth, stay alert to symptoms that suggest your numbers might not reflect your reality. If you feel well, have normal daily readings, but see an unexpected HbA1c, do not panic. Get a cross-check. If your HbA1c runs high but your CGM and fructosamine are normal, it could be a biological difference, not a sign of hidden risk.
Finally, keep your provider in the loop. Share your logs, ask questions about lab methods, and advocate for repeat or alternative testing when needed. You are not just a number—you are a person with a unique biology, and your health strategy should reflect that. Next, let’s talk about lifestyle levers that support healthy glucose and make the most of your tracking efforts.
Numbers are only part of the story. The way you eat, move, and sleep all show up in your glucose patterns—sometimes more dramatically than any pill or supplement. Here’s how to make lifestyle choices that help keep your time-in-range high and your risk low, no matter what your HbA1c says.
Start with nutrition. Meals that are high in refined carbohydrates and sugars cause rapid spikes in blood glucose. Pairing carbohydrates with protein, fiber, and healthy fats slows down absorption and blunts those spikes. For example, adding beans or leafy greens to a pasta dish can flatten your glucose curve. Experiment with meal timing, too. Some people find that eating larger meals earlier in the day and having lighter dinners reduces overnight glucose surges. The Mediterranean-style diet, rich in vegetables, whole grains, nuts, olive oil, and fish, is backed by decades of research for glucose stability and lower risk of complications.
Movement is your metabolic ally. Even light activity after meals can reduce glucose spikes. Try to walk for ten to fifteen minutes within thirty minutes of eating. This simple habit activates glucose transporters in your muscles, pulling sugar out of your blood without extra insulin. Resistance training—using weights, bands, or your body weight—builds muscle, which increases your capacity to store and use glucose. Aim for at least two sessions per week. If you are new to exercise, start small and build up gradually. Every bit counts.
Sleep matters more than most people realize. Short or disrupted sleep can increase insulin resistance and make your blood sugar harder to control. Adults should aim for seven to nine hours of quality sleep per night. If you struggle with sleep, work on a consistent bedtime, limit screens before bed, and keep your room dark and cool. Stress management is another hidden driver. Chronic stress hormones, especially cortisol, can raise your glucose independently of what you eat. Mindfulness, deep breathing, or even a few minutes outdoors can help reset your system.
These lifestyle levers do not just improve your numbers—they reshape your biology. They make your body more resilient to the quirks of HbA1c and help you build a foundation for long-term health. Up next, let’s talk about early warning signs that your numbers or symptoms deserve a closer look.
You do not need to wait for a lab test to know when something is off. Your body often sends signals before the numbers show trouble. Paying attention to these early warning signs can help you catch hidden metabolic issues—or spot when your lab results are out of sync with your lived reality.
Watch for energy crashes, especially after meals. If you feel sleepy, irritable, or shaky a couple of hours after eating, your glucose might be spiking and dropping more than you realize. If you find yourself needing frequent snacks or craving sweets in the afternoon, that is a clue that your glucose regulation could use some attention.
Notice any unexplained changes in your vision, tingling in your hands or feet, or wounds that heal slowly. These can be signs of glucose swings or chronic high blood sugar—even when your HbA1c looks normal. Likewise, sudden shifts in your weight, either up or down, without changes in your eating or activity, can point to hidden metabolic stress.
If you have a family history of anemia, hemoglobin variants, or blood disorders, let your doctor know. These conditions can make your HbA1c results less reliable and put you at risk for missed diagnoses or inappropriate treatment. The same goes for recent blood loss, transfusions, or kidney disease.
If you use a fingerstick meter or CGM and see a consistent gap between your daily readings and your HbA1c, treat that as a reason to ask for a cross-check. If your symptoms and your numbers are not matching up, push for a fructosamine or glycated albumin test.
And if your doctor seems overly focused on a single lab result that does not fit your experience, speak up. Share your logs, ask about your biology, and remember that you are the expert on how you feel day to day.
Catching these early warning signs is not about fear—it is about empowerment. The sooner you recognize a mismatch, the sooner you can get a true picture and take action.
It is easy to put too much trust in a single health number, especially when it is as widely used as HbA1c. But as you have heard, this marker is shaped by your genetics, your red blood cell biology, and even the technology used at your lab. One number cannot tell your whole story.
The most important lesson is this: you have tools and choices. Combining HbA1c with CGM, fingerstick logs, and alternative markers like fructosamine and glycated albumin can give you a much clearer, more accurate picture. Track your time-in-range and look for patterns, not just averages. Use lifestyle levers—nutrition, movement, sleep, and stress management—to keep your glucose steady and your risk low.
If your numbers do not match your experience, do not settle for confusion. Ask for cross-checks, repeat testing, and seek out a provider who understands the complexity of metabolic health. Personalize your tracking and your interventions to fit your unique biology. Remember, you are not just a lab result—you are a whole person, and your health story is yours to write.
The next step is simple. Take stock of your current markers, look for any mismatches or unexplained results, and have a conversation with your healthcare provider about the best way to get a true read on your metabolic health. The more you understand your numbers, the better equipped you are to take action and protect your long-term vitality.
Your HbA1c Number May Be Lying to You — And Genetics Explains Why
Up to 40% of people have systematic differences between their HbA1c and actual glucose exposure
Diagram glossary
- CGM:
- A wearable device that continuously monitors blood sugar levels throughout the day.
- DNA:
- The genetic material that can contain variants affecting red blood cell biology and HbA1c.
- eAG:
- Estimated average glucose, a metric translating HbA1c into an average blood sugar level.
- fructosamine:
- A diagnostic blood test used to measure average glucose levels over a few weeks.
- Glucose:
- A simple sugar in the blood that attaches to hemoglobin over time.
Conclusions
HbA1c is useful, but it is not a universal truth. Your red blood cell lifespan, hemoglobin type, and test method can push HbA1c up or down without a real change in glucose. If your HbA1c does not match your CGM or meter patterns, do not guess. Add fructosamine or glycated albumin, and use CGM time-in-range to see both average glucose and swings.
Exact red blood cell lifespans are rarely measured in routine care, so discordance is often inferred from patterns, not proven directly. Many studies on HbA1c discordance and genetics are observational, and do not prove cause for every person. Fructosamine and glycated albumin can also be biased by protein-related issues (like low albumin) and may vary by lab. CGM accuracy depends on sensor type and proper use, and targets like time-in-range can differ by age, pregnancy, and comorbidities.
Track this in your stack
See how hba1c relates to your health goals and monitor changes in your biomarkers over time.
Sources (7)
This article informs how supplementation moves 1 marker.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.