
Your Vitamin K2 Supplement May Be Working—But Not Where You Think It Is
Why measuring osteocalcin carboxylation determines whether you'll see metabolic benefits from K2
The surprising truth: vitamin K2 can change your blood markers fast, yet you may feel no difference.
Most people think lower ucOC means K2 “worked.” That is only step one. The bigger question is this: did your osteocalcin change enough to shift metabolism? In one 3-year trial, only stronger responders saw a rise in adiponectin.
What this means for you is simple. You should not guess. You can test if you respond. If your ucOC drops a lot, you may also see better insulin markers. If it barely drops, your dose, absorption, or cofactors may be the issue.
Start with MK-7 at 180–360 mcg daily with a fat-containing meal. Retest ucOC in 8–12 weeks. If ucOC barely moves, consider 720 mcg daily, used in trials. Track every 6 months once stable.
- MK-7
- Menaquinone-7, a common supplemental K2 form with a long half-life, often dosed in micrograms (mcg).
- Randomized controlled trial (RCT)
- A study where people are randomly assigned to a supplement or placebo group to test cause and effect.
- Adiponectin
- Protective adipokine that enhances insulin sensitivity and reduces inflammation. low levels predict type 2 diabetes and cardiovascular disease.
- dp-ucMGP
- Dephosphorylated-uncarboxylated MGP. A sensitive marker of low vitamin K status in the vascular system; it usually falls with K2.
- Vitamin K2 (menaquinones)
- A family of vitamin K forms (MK-4, MK-7, and others) used to activate vitamin K–dependent proteins.
- Hemoglobin A1c
- Average blood sugar over the past 2-3 months by assessing glycated hemoglobin. each 1% increase raises cardiovascular risk by 18%.
- HOMA-IR (calc)
- Insulin resistance by combining fasting glucose and insulin levels.
- AVADEC
- A clinical trial evaluating the impact of Vitamin K2 on arterial calcification.
- insulin
- A metabolic hormone whose markers may improve following a significant drop in ucOC.
- osteocalcin
- A key bone protein that requires Vitamin K2 for its activation.
The Protein Activation Paradox
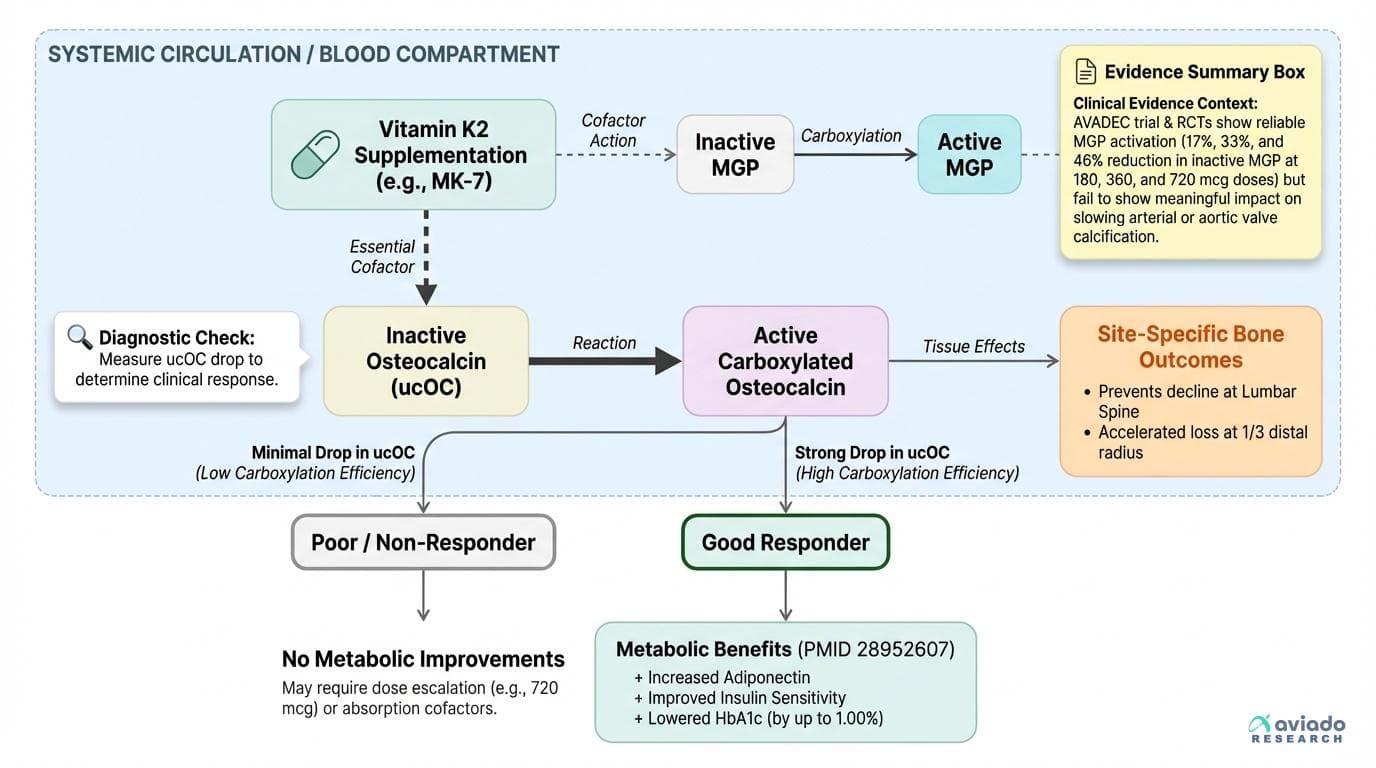
Vitamin K2 excels at one thing: activating vitamin K-dependent proteins. Meta-analyses spanning over 6,000 participants consistently show that K2 supplementation reduces undercarboxylated osteocalcin, the inactive form of a key bone protein [1]. In hemodialysis patients, an 8-week dose-finding trial demonstrated that MK-7 doses of 180, 360, and 720 μg daily reduced inactive MGP (a vascular protein) by 17%, 33%, and 46% respectively [2]. The protein activation is dose-dependent and remarkably reliable.
Yet when researchers track actual clinical outcomes, the picture becomes murky. A 24-month randomized trial of 365 patients found that MK-7 720 μg daily plus vitamin D successfully activated calcification-inhibiting proteins but failed to slow aortic valve calcification progression compared to placebo [3]. Similarly, the AVADEC trial substudy showed reduced dp-ucMGP levels but no meaningful impact on arterial calcification [4]. The proteins get activated, but the expected downstream benefits often don't materialize.
This disconnect suggests that protein activation alone isn't sufficient—there's an additional layer determining who actually benefits from these biochemical changes.
The Responder/Non-Responder Discovery
The breakthrough came from a 3-year study that looked beyond simple protein activation to examine who actually gained metabolic benefits. Researchers found that only participants with above-median osteocalcin carboxylation responses showed increases in adiponectin, a hormone crucial for insulin sensitivity and metabolic health [5]. Those with below-median carboxylation responses activated their proteins just as effectively but saw no metabolic improvements.
This finding reframes vitamin K2 from a universal supplement to a precision tool. The same 360 μg dose that produces dramatic metabolic improvements in good responders may be metabolically inert in poor responders, even though both groups show similar ucOC reduction on paper. Without measuring your individual carboxylation response, you're supplementing blind.
The responder pattern appears most pronounced for metabolic outcomes. Meta-analyses show that K2 reduces HbA1c by 1.00% in some studies [6], while others find minimal effects in healthy populations. The difference likely lies in baseline insulin resistance and individual carboxylation efficiency—two factors that standard K2 marketing completely ignores.
Population-Specific Effects: Why Context Matters
Recent evidence suggests K2 effects depend on who you are and what you need. In a 12-week randomized trial in insulin-independent type 2 diabetes (n=68), K2 improved blood sugar control, with HbA1c dropping significantly versus placebo (p=0.004) [7]. In healthier groups, many trials show smaller or no metabolic shifts, likely because baseline glucose control is already good.
Bone outcomes also look site-specific. In a 2-year double-blind trial (n=123), MK-7 at 360 mcg/day sped up bone mineral density loss at the 1/3 distal radius, while it prevented decline at the lumbar spine [8]. That split result suggests “bone benefit” is not one simple outcome.
For arteries and valves, several trials show a consistent pattern: K2 lowers dp-ucMGP, but imaging endpoints often do not move. In a 24-month trial in aortic valve calcification (n=365), MK-7 720 mcg/day plus vitamin D improved vitamin K status markers but did not slow calcification progression versus placebo [3].
Dosing for Individual Response
The dose-response data reveals why many people see minimal benefits from standard K2 supplements. The 8-week hemodialysis trial showed that 180 μg of MK-7—close to typical supplement doses—produced only modest protein activation [2]. Meaningful biochemical changes required 360-720 μg daily, doses 3-7 times higher than most commercial formulations.
For metabolic benefits, the effective dose appears to be 360 μg of MK-7 daily, based on successful trials in diabetes patients [7][8]. However, this assumes you're a good responder. Poor responders may need higher doses, better cofactor status (vitamin D and magnesium), or may simply lack the genetic machinery to convert K2's protein effects into metabolic benefits.
The timing and context of supplementation also matter. K2 is fat-soluble and absorption improves significantly when taken with meals containing fats. Some studies suggest that vitamin D status influences K2 effectiveness, though the optimal ratio remains unclear. What's certain is that the standard approach of taking 100-200 μg daily without measuring response is unlikely to produce meaningful benefits in most people.
Testing Your K2 Response
You can’t judge K2 by dose alone. You need a response marker. The simplest approach is to track ucOC.
Test total osteocalcin and ucOC before you start. Then retest after 8–12 weeks on a steady dose. A strong responder shows a clear ucOC drop and a better carboxylated-to-undercarboxylated pattern.
If your goal is metabolic support, add HbA1c and consider adiponectin. These reflect the outcomes people care about most. If your ucOC barely changes, focus on basics that affect K2 use: take MK-7 with a fat-containing meal, and check vitamin D and magnesium status. Trials have used MK-7 up to 720 mcg/day, but the key is whether your ucOC actually moves.
Your Vitamin K2 Supplement May Be Working—But Not Where You Think It Is
Why measuring osteocalcin carboxylation determines whether you'll see metabolic benefits from K2
Diagram glossary
- adiponectin:
- A metabolic protein whose levels may rise in strong responders to Vitamin K2.
- AVADEC:
- A clinical trial evaluating the impact of Vitamin K2 on arterial calcification.
- insulin:
- A metabolic hormone whose markers may improve following a significant drop in ucOC.
- MK-7:
- A specific, highly bioavailable form of Vitamin K2 used in clinical supplementation trials.
- osteocalcin:
- A key bone protein that requires Vitamin K2 for its activation.
- Responder/Non-Responder:
- A classification indicating whether a patient exhibits clinical benefits from a specific treatment.
- ucMGP:
- The inactive, undercarboxylated form of matrix Gla protein, a vascular calcification inhibitor.
- ucOC:
- The inactive, undercarboxylated form of osteocalcin that decreases with Vitamin K2 supplementation.
- Vitamin K2:
- A nutrient that activates specific proteins involved in bone and vascular health.
Conclusions
Vitamin K2 reliably improves vitamin K status markers, but health outcomes vary. The big divider seems to be response size, not just the label dose. If you want metabolic benefits, your best bet is to measure ucOC, then match your dose to your personal change. For bone, results can differ by site. For arterial and valve calcification, trials often show better dp-ucMGP without clear imaging changes. The practical takeaway is simple: test, supplement, retest, then decide.
The responder vs non-responder idea relies on a small number of long trials and needs more replication. ucOC tests are not fully standardized across labs, so results may not match between providers. Many studies focus on postmenopausal women, type 2 diabetes, or hemodialysis populations, so results may not generalize to all healthy adults. Higher-dose safety data (up to 720 mcg/day MK-7) mainly comes from controlled trials, not long-term open use.
Track this in your stack
See how vitamin k2 relates to your health goals and monitor changes in your biomarkers over time.