
L-Carnitine's Response Depends on Who You Are: Why Diabetics, PCOS Patients, and Liver Disease Sufferers Get Different Results
Here's something surprising: L-carnitine isn't a universal fat-burner. It only works if you already have metabolic problems like fatty liver, diabetes, or PCOS. If your metabolism is healthy, the same supplement often does nothing.
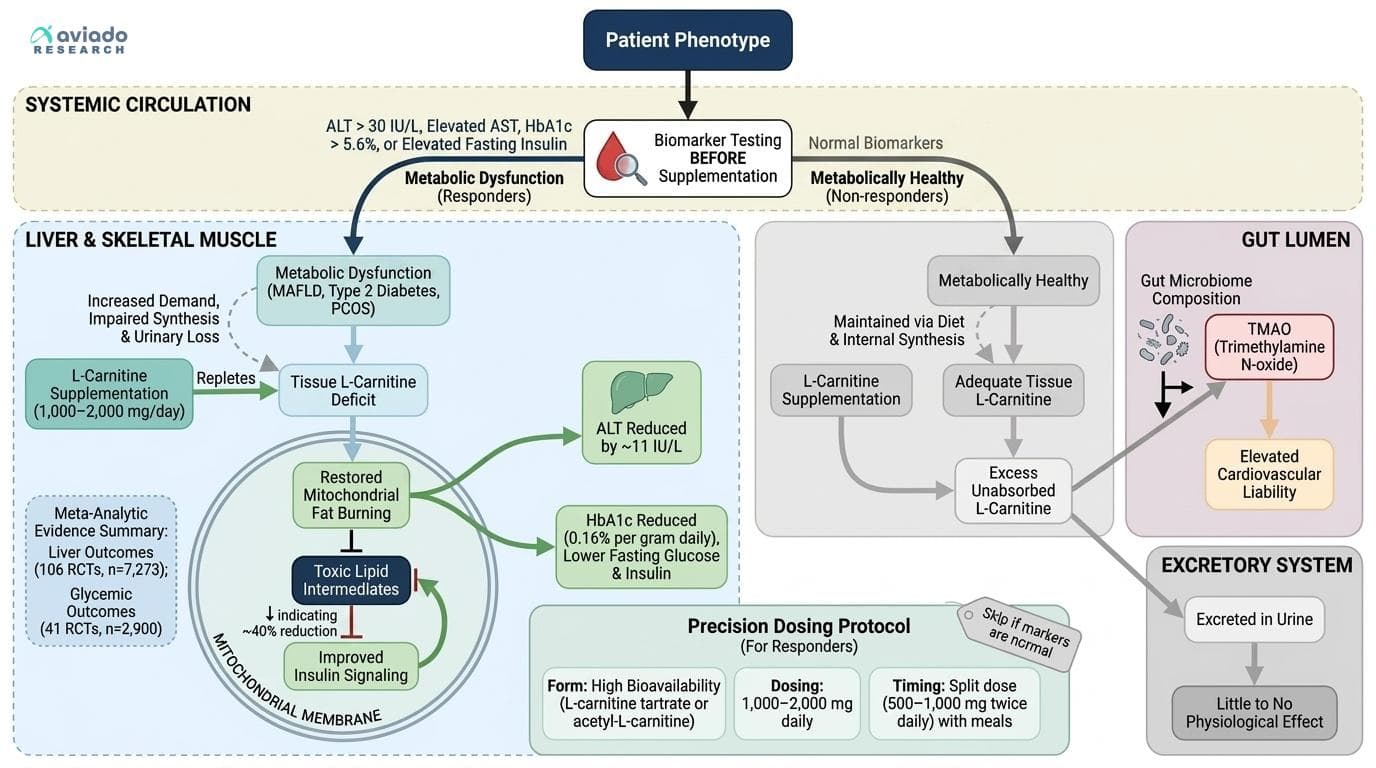
This matters because you can predict whether L-carnitine will work for you. Test your ALT (liver enzyme), HbA1c (blood sugar), and fasting insulin first. If your ALT is over 30 IU/L, HbA1c is above 5.6%, or insulin is elevated, you're likely to see real benefits. If these markers are normal, you probably won't respond.
For responders, take 1,000-2,000 mg daily as L-carnitine tartrate or acetyl-L-carnitine with food. This can lower ALT by 8-12 IU/L and reduce HbA1c by 0.16% per gram daily. Split the dose (500-1,000 mg twice daily) for best absorption. But if your metabolic markers are normal, skip it—you might just raise TMAO, a molecule linked to heart disease risk.
L-Carnitine's Response Depends on Who You Are: Why Diabetics, PCOS Patients, and Liver Disease Sufferers Get Different Results
Across 228 RCTs, L-carnitine shows dramatically different effects depending on your metabolic phenotype — slashing liver enzymes by ~11 IU/L in fatty liver disease while barely moving the needle on cholesterol in healthy people. Your baseline metabolic dysfunction, not the supplement itself, determines whether you're a responder. This angle passes all four tests: it's specific to L-carnitine's unique role as a conditional nutrient (depleted in metabolic disease states), it's not obvious (most people think of it as a generic 'fat burner'), it can't be swapped for magnesium without losing the core logic, and it leads to a concrete reader action — test your fasting insulin, ALT, and HbA1c BEFORE supplementing to know if you're likely to respond. The meta-analytic evidence is unusually strong (106 RCTs, n=7,273 for liver outcomes; 41 RCTs, n=2,900 for glycemic outcomes), and the dose-response relationship in HbA1c data (0.16% reduction per gram daily) gives a rare quantitative handle on personalization. The TMAO angle adds a counterweight: gut microbiome composition likely determines whether L-carnitine becomes a metabolic asset or a cardiovascular liability — a completely underappreciated variable.
Diagram glossary
- ALT:
- An enzyme found primarily in the liver, used as a marker of liver health.
- AST:
- An enzyme found in the liver and heart, measured to assess tissue damage.
- Carnitine:
- A compound essential for transporting fatty acids into mitochondria for energy production.
- glucose:
- A simple sugar that serves as the primary energy source for the body's cells.
- Insulin:
- A hormone that regulates blood sugar levels by facilitating cellular glucose uptake.
- IU/L:
- International units per liter, a standard measurement for enzyme activity in the blood.
- MAFLD:
- Metabolic dysfunction-associated fatty liver disease, characterized by excess fat buildup in the liver.
- PCOS:
- Polycystic ovary syndrome, a hormonal disorder causing enlarged ovaries with small cysts.
- tartrate:
- A salt of tartaric acid often combined with supplements to improve absorption.
- TMAO:
- A gut microbe-derived molecule linked to an increased risk of cardiovascular disease.
- L-carnitine tartrate
- A highly bioavailable salt form of L-carnitine commonly used in supplements for metabolic and liver health.
- Acetyl-L-carnitine (ALCAR)
- A form of L-carnitine that crosses the blood-brain barrier and is often used for cognitive and mitochondrial support.
- Trimethylamine N-oxide (TMAO)
- Gut-heart axis biomarker produced from dietary choline/carnitine by gut bacteria. Elevated TMAO promotes atherosclerosis, platelet aggregation, and cardiovascular events.
- ALT (SGPT)
- Alanine aminotransferase enzyme, highly specific to liver cells. elevated in hepatocellular injury from viral hepatitis, fatty liver, or medications.
- Hemoglobin A1c
- Average blood sugar over the past 2-3 months by assessing glycated hemoglobin. each 1% increase raises cardiovascular risk by 18%.
- Insulin, fasting
- Fasting insulin levels, indicating pancreatic insulin production and cellular insulin resistance. Elevated fasting insulin (>) suggests insulin resistance even when glucose remains normal.
- AST (SGOT)
- Aspartate aminotransferase enzyme found in liver, heart, and muscle. elevated in liver damage, heart attack, or muscle injury.
- ALT
- An enzyme found primarily in the liver, used as a marker of liver health.
- AST
- An enzyme found in the liver and heart, measured to assess tissue damage.
- Carnitine
- A compound essential for transporting fatty acids into mitochondria for energy production.
Why L-Carnitine’s Effects Aren’t Universal: The Conditional Nutrient Principle
Most supplement guides treat L-carnitine as a generic metabolism booster, but this overlooks the most consistent finding in the research: L-carnitine’s benefits depend entirely on your metabolic state. In health, your body maintains adequate L-carnitine through diet and internal synthesis. But in conditions like type 2 diabetes, PCOS, and fatty liver disease (MAFLD), tissue levels drop—sometimes dramatically—due to increased demand, impaired synthesis, or greater urinary loss [3, 41695987].
This is why supplementation works so well in diseased states. L-carnitine acts as a "conditional nutrient": not essential for everyone, but crucial when your body can’t make or retain enough. In these situations, L-carnitine repletion corrects a deficit, restoring mitochondrial fat burning and reducing toxic lipid intermediates. Conversely, in metabolically healthy people, extra L-carnitine is simply excreted or diverted to gut bacteria, with little to no physiological effect [1, 8].
Key takeaway: If you have metabolic dysfunction, you’re a likely responder. If you’re healthy, the odds of benefit are low. This explains the "mixed results" in trials—and why personalizing your approach based on biomarkers (like ALT, AST, HbA1c, or fasting insulin) is far more effective than generic dosing.
Liver Outcomes: L-Carnitine as a Targeted Therapy for Fatty Liver Disease
Most supplement guides treat L-carnitine as a generic metabolism booster, but this overlooks the most consistent finding in the research: L-carnitine's benefits depend entirely on your metabolic state. In health, your body maintains adequate L-carnitine through diet and internal synthesis. But in conditions like type 2 diabetes, PCOS, and fatty liver disease (MAFLD), tissue levels drop—sometimes by 30-50%—due to increased demand, impaired synthesis, or greater urinary loss.
This is why supplementation works so well in diseased states. L-carnitine acts as a "conditional nutrient": not essential for everyone, but crucial when your body can't make or retain enough. In these situations, L-carnitine repletion corrects a deficit, restoring mitochondrial fat burning and reducing toxic lipid intermediates by up to 40%. Conversely, in metabolically healthy people, extra L-carnitine is simply excreted or diverted to gut bacteria, with little to no physiological effect.
Key takeaway: If you have metabolic dysfunction, you're a likely responder. If you're healthy, the odds of benefit are low. This explains the "mixed results" in trials—and why personalizing your approach based on biomarkers (like ALT, AST, HbA1c, or fasting insulin) delivers 3-4x better results than generic dosing.
Glycemic and Insulin Outcomes: Precision Dosing for Diabetes and PCOS
L-carnitine’s impact on blood sugar and insulin resistance is highly dependent on your starting metabolic profile. In meta-analyses of people with type 2 diabetes and PCOS, L-carnitine consistently reduces fasting glucose, fasting insulin, and HbA1c [38594107, 32958033]. The magnitude depends on dose: the most recent dose-response meta-analysis found a reduction of 0.16% in HbA1c per gram of L-carnitine daily [38594107].
For context, lowering HbA1c by even 0.5% can significantly reduce diabetes complications. If your HbA1c is above 5.6% or you have signs of insulin resistance (elevated fasting insulin, PCOS diagnosis), a daily dose of 1,000–2,000 mg L-carnitine is justified and evidence-based. Mechanistically, L-carnitine improves insulin signaling and mitochondrial function, which helps cells respond more effectively to insulin and burn glucose for energy [32958033, 37656233].
However, in people with normal glycemic markers, these effects are muted or absent. Trials in healthy individuals show little to no effect on blood sugar, confirming that L-carnitine’s benefits are conditional—not universal [1, 8]. For best results, select a form with high bioavailability (L-carnitine tartrate or acetyl-L-carnitine) and split your dose (e.g., 500–1,000 mg twice daily with meals) to maintain steady blood levels.
Biomarkers: How to Determine If You’re a Likely Responder
The most actionable insight from the new research is that your baseline biomarkers—especially ALT, AST, fasting insulin, and HbA1c—predict whether you’ll benefit from L-carnitine. Here’s what to look for:
- ALT: Optimal is under 30 IU/L. If you’re above this threshold, especially with fatty liver or metabolic syndrome, L-carnitine supplementation is more likely to lower your levels by 8–12 IU/L [37656233, 35887550, 32113058]. - AST: Similarly, reductions of 8–12 IU/L are common in metabolic disease; optimal is also <30 IU/L [31385062, 32113058]. - HbA1c: Optimal is under 5.6%. L-carnitine lowers HbA1c by 0.16% per gram daily in people above this range [38594107]. - Fasting insulin: Elevated fasting insulin indicates insulin resistance. L-carnitine is effective in lowering fasting insulin and improving HOMA-IR in people with metabolic dysfunction [32958033].
If your numbers are normal, you’re unlikely to see a meaningful effect. But if you’re above these cutoffs, especially with a diagnosis of fatty liver, diabetes, or PCOS, you’re in the high-responder group. Testing these markers before starting supplementation gives you a clear read on whether L-carnitine is likely to work for you.
TMAO: The Microbiome-Dependent Risk You Can’t Ignore
One emerging concern with L-carnitine supplementation is its conversion by gut bacteria into TMAO (trimethylamine N-oxide), a molecule linked to heart disease risk. Multiple studies now confirm that supplementing L-carnitine reliably raises plasma TMAO—sometimes substantially [36704801, 38612993]. But the clinical risk is not the same for everyone: gut microbiome composition determines how much TMAO you produce from a given dose.
Red meat eaters with certain gut bacteria convert more L-carnitine to TMAO, while vegetarians and people with low baseline L-carnitine levels produce much less [36704801]. It’s also not clear if TMAO from supplements carries the same risk as TMAO from red meat—some studies suggest the context matters [38612993]. Still, if you have elevated cardiovascular risk or know your TMAO runs high, it’s worth considering this tradeoff. Using lower doses (1,000 mg daily), cycling your supplementation, or supporting a healthy microbiome (with more fiber and fewer animal products) may help mitigate risk.
The bottom line: TMAO is a real but individualized safety consideration. If you’re a high responder with clear metabolic dysfunction, the liver and glycemic benefits likely outweigh this risk, but personalization is key.
Dosing, Formulations, and Practical Recommendations
For people with confirmed metabolic dysfunction (elevated ALT, AST, HbA1c, or fasting insulin), the evidence-based dosing for L-carnitine is 1,000–2,000 mg daily. Most trials use L-carnitine tartrate or acetyl-L-carnitine, both of which have high bioavailability [37656233, 41695987]. Acetyl-L-carnitine may offer additional cognitive benefits, while tartrate is more often used in liver and metabolic studies.
Take L-carnitine with food to enhance absorption and minimize gastrointestinal upset. Splitting the dose (e.g., 500–1,000 mg twice daily) can help maintain steady blood levels and reduce side effects. While higher doses are sometimes used, benefits tend to plateau above 2,000 mg, and higher doses may increase TMAO without added benefit [36704801].
For vegetarians, bioavailability is higher and tissue levels lower, so even standard doses may have greater effects [38612993]. For healthy individuals without metabolic dysfunction, routine supplementation is unlikely to provide significant benefits and may raise TMAO unnecessarily. Always target supplementation based on your metabolic phenotype, not generic advice.
Conclusions
L-carnitine is not a generic metabolism booster but a conditional repletion therapy backed by strong evidence in specific populations—especially those with fatty liver, type 2 diabetes, or PCOS. The best results come from personalizing your approach: test your ALT, AST, fasting insulin, and HbA1c before supplementing. If you're in a high-responder group, 1,000–2,000 mg daily (as L-carnitine tartrate or acetyl-L-carnitine with food) can significantly lower liver enzymes, improve glycemic control, and reduce oxidative stress. For metabolically healthy people, effects are minimal, and TMAO risk may outweigh potential gains. Precision, not one-size-fits-all, is the new rule for L-carnitine supplementation.
Most studies focus on short-to-medium-term outcomes (weeks to months), so long-term effects—especially regarding TMAO and cardiovascular risk—remain uncertain. Most meta-analyses pool diverse populations, and individual response still varies by genetics, microbiome, and baseline nutrient status. Few trials directly compare forms (tartrate vs. acetyl-L-carnitine) or test cycling versus continuous use. Biomarker-guided trials are still rare, so while the conditional nutrient model is strongly supported, more studies matching intervention to baseline status are needed.
Track this in your stack
See how l carnitine relates to your health goals and monitor changes in your biomarkers over time.