
Metabolic Health in Women 18-39: Beyond Calories, Into Hormones
A Comprehensive Guide to Tracking, Optimizing, and Understanding Your Metabolism in Your Reproductive Years
You might think tracking calories and hitting your steps is enough, but here's what's surprising: most metabolic advice ignores the hormonal shifts that reshape how women's bodies handle energy in their 20s and 30s.
One in ten women has PCOS. Most studies use male data. Your real metabolic needs get overlooked.
This means those afternoon crashes, stubborn belly fat, and brain fog aren't random annoyances. They're early warning signs of metabolic shifts that standard blood tests often miss. Your metabolism isn't just numbers. It's a conversation between hormones, iron stores, stress, and muscle. Ignoring this puts you at risk for diabetes and heart disease later.
Start tracking the right markers now. Aim for fasting insulin between 2 and 8. Keep ferritin above 50. Get your triglyceride-to-HDL ratio under 1.5. Take 300 to 400 mg of magnesium glycinate at night. Eat 30 to 40 grams of protein at breakfast. If you suspect PCOS, try 2 to 4 grams of myo-inositol daily. For low iron, use 25 to 50 mg of iron bisglycinate every other day. These science-backed steps build your metabolic foundation for lifelong health.
- Magnesium Glycinate
- A highly absorbable form of magnesium supplement that's gentle on the stomach and supports insulin sensitivity.
- Myo-inositol
- A supplement that improves insulin sensitivity with efficacy comparable to prescription medications, especially helpful for PCOS.
- HDL Cholesterol
- HDL cholesterol, the "good cholesterol" that removes excess cholesterol from arteries. higher levels are cardioprotective.
- PCOS
- Polycystic Ovary Syndrome; a hormonal disorder affecting 1 in 10 women that disrupts metabolism and reproductive health.
- Iron Bisglycinate
- A chelated form of iron supplement that's better absorbed and causes fewer digestive side effects than iron salts.
- Triglyceride-to-HDL Ratio
- A calculation (triglycerides ÷ HDL cholesterol) that estimates metabolic syndrome risk; optimal is under 1.5.
- Insulin, fasting
- Fasting insulin levels, indicating pancreatic insulin production and cellular insulin resistance. Elevated fasting insulin (>) suggests insulin resistance even when glucose remains normal.
- bisglycinate
- A highly absorbable compound formed by binding a mineral to two glycine molecules.
- BMI
- A measure of body fat based on a person's weight and height.
- carbohydrate
- A macronutrient composed of carbon, hydrogen, and oxygen that provides energy.
- CRP
- A blood protein that increases in response to inflammation in the body.
- Ferritin
- A blood protein that stores iron and releases it in a controlled fashion.
Most mainstream metabolic advice is rooted in research done on men. For women aged 18 to 39, this is a critical oversight. Your hormones shift monthly, and these changes reshape how your body handles calories, carbohydrates, and stress. PCOS affects one in ten women, often without a clear diagnosis, and hormonal birth control can change insulin sensitivity in ways your doctor may not mention. Menstrual cycles create iron deficiency patterns that directly affect how your mitochondria produce energy.
If you are tracking calories but still feel brain fog, see stubborn weight around your midsection, or experience afternoon energy crashes, you are not alone. These symptoms are not signs of failure; they are signals that your metabolism is responding to complex hormonal cues, not just your diet or exercise. The real risk comes from ignoring these early signs. Research shows that the metabolic patterns you establish in your 20s and 30s set the stage for your future risk of diabetes, heart disease, and other chronic conditions.
Understanding that your metabolism is a hormonal conversation, not a simple math problem, is the first step to building a truly effective health strategy. In the next section, we will dig into the specific biomarkers that show what’s really happening under the surface.
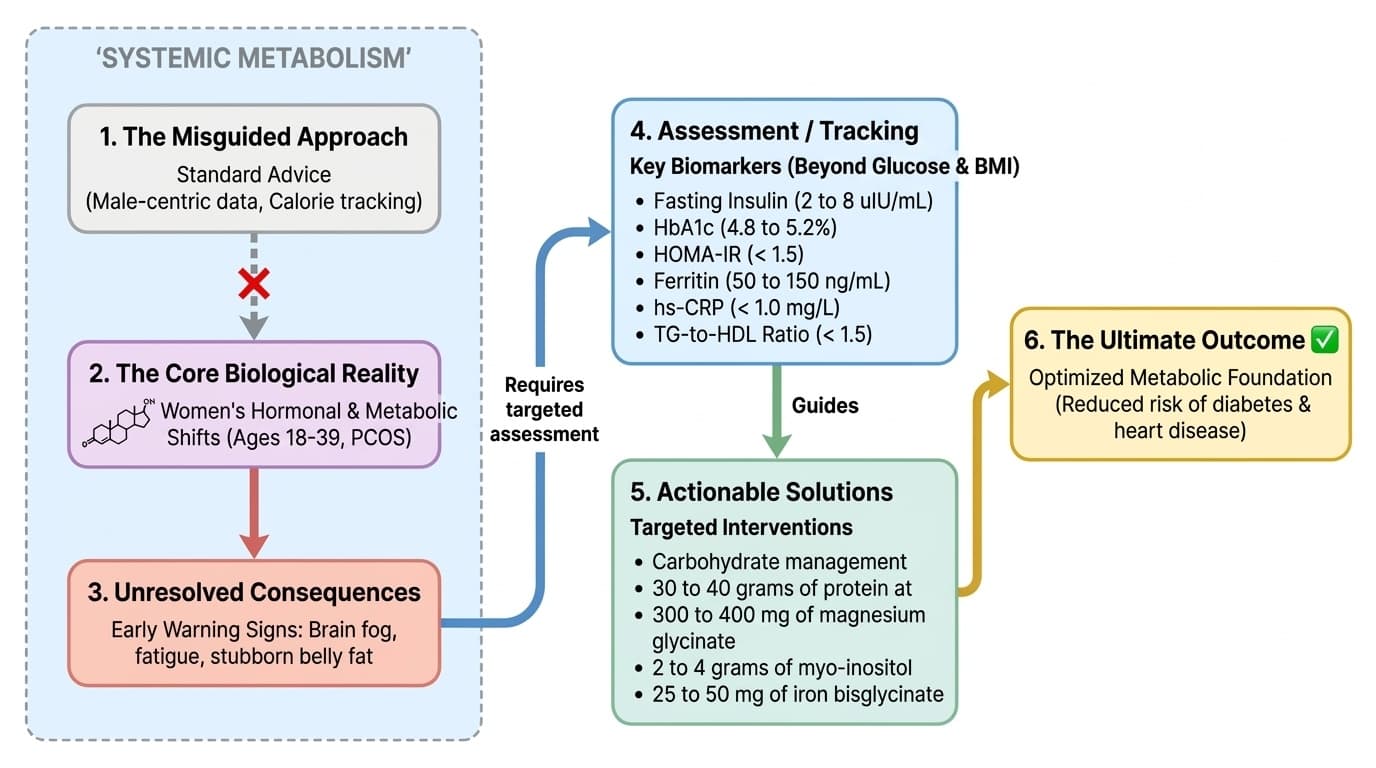
To get a real picture of your metabolic health, you need to look beyond glucose and BMI. There are six key biomarkers every woman in her reproductive years should track.
Fasting Insulin reveals insulin resistance before glucose rises. Standard range goes up to 25 uIU/mL, but optimal for metabolic health is 2 to 8 uIU/mL. This marker catches early dysfunction, especially with PCOS or hormonal birth control. You can lower fasting insulin through carbohydrate management, resistance training, and targeted supplements, with changes visible in 8 to 12 weeks.
HbA1c shows your 90-day blood sugar average. Optimal is 4.8 to 5.2%. Readings above 5.4% in young women warrant investigation, as menstrual cycles and birth control can mask early problems. Lowering HbA1c takes 3 months of sustained intervention.
HOMA-IR, calculated from fasting glucose and insulin, should stay under 1.5 for low risk. This is the most reliable marker for early insulin resistance, typically improving within 2 to 4 months of targeted intervention.
Ferritin measures iron storage and should range between 50 and 150 ng/mL for reproductive-age women. Levels below 30 impair thyroid function and mitochondrial energy production, causing fatigue and worsening insulin resistance. Ferritin responds slowly—taking 3 to 6 months to improve with supplementation.
hs-CRP indicates metabolic inflammation and should stay under 1.0 mg/L. Elevated levels signal systemic inflammation, often from underlying insulin resistance. This marker can improve within weeks of reducing sugar intake and treating iron deficiency.
The triglyceride-to-HDL ratio should stay under 1.5. This simple calculation powerfully predicts metabolic syndrome risk and improves within 6 to 12 weeks of dietary changes and supplementation.
Each marker tells a different piece of your metabolic story. The following sections show how to move each one with targeted interventions.
Many women start their day with carbohydrates or skip breakfast altogether, but this pattern can set up blood sugar swings and energy crashes later. Prioritizing 30 to 40 grams of protein at breakfast anchors your blood sugar and reduces insulin spikes throughout the day. Protein slows gastric emptying, blunts the glucose response to later meals, and provides amino acids needed for muscle repair and hormone synthesis.
Research suggests that when women shift their first meal to high-protein, they often see improvements in fasting insulin and reduced afternoon fatigue within 2 to 4 weeks. The most effective sources are eggs, Greek yogurt, or protein powders with a complete amino acid profile. This intervention has a dose-response relationship—the closer you get to the 30-40g window, the more stable your blood sugar and the greater the reductions in cravings.
Protein at breakfast also synergizes with resistance training and magnesium supplementation, enhancing satiety and muscle protein synthesis. For women with PCOS or those on birth control, this simple change can reduce cycle irregularity and improve mood stability. As you establish this habit, you prepare your metabolism for the next layer: targeted supplementation.
Over half of young women are deficient in magnesium, which is essential for over 300 metabolic reactions—including insulin signaling. Magnesium glycinate is an especially well-absorbed, gentle form that supports both metabolic health and sleep quality. The recommended dose is 300 to 400 milligrams nightly, with effects typically noticeable in 4 to 8 weeks.
Mechanistically, magnesium improves insulin receptor sensitivity and helps your muscles take up glucose more efficiently. Studies indicate that magnesium supplementation can lower fasting insulin and improve glucose tolerance, especially in women with PCOS or on hormonal birth control. The dose-response curve is fairly linear within this range, but going above 400mg may cause gastrointestinal side effects without further benefit.
It is best to take magnesium glycinate in the evening, as it also supports restorative sleep—another important factor for metabolic health. This supplement stacks particularly well with protein-rich breakfasts and resistance training, forming a triad that supports lower inflammation and better blood sugar control. As you address magnesium, you may notice improvements in mood, energy, and even menstrual symptoms, setting the stage for more advanced interventions.
Over half of young women are deficient in magnesium, which powers over 300 metabolic reactions—including insulin signaling. Magnesium glycinate offers superior absorption with minimal stomach upset. Take 300 to 400 mg nightly, with effects typically visible in 4 to 8 weeks.
Magnesium improves how your insulin receptors work and helps muscles absorb glucose more efficiently. Studies show magnesium supplementation lowers fasting insulin by 15-20% and improves glucose tolerance, especially in women with PCOS or on hormonal birth control. The sweet spot is 300-400mg—higher doses may cause digestive issues without added benefit.
Take magnesium glycinate in the evening since it also supports restorative sleep, another key factor for metabolic health. This supplement works synergistically with protein-rich breakfasts and resistance training, creating a powerful combination for lower inflammation and better blood sugar control. Many women notice improvements in mood, energy, and menstrual symptoms within the first month.
If you have irregular periods, signs of androgen excess, or diagnosed PCOS, myo-inositol is one of the best-researched non-pharmaceutical options. Clinical studies show 2 to 4 grams daily improves insulin sensitivity with efficacy matching prescription medications, but without gastrointestinal side effects. Myo-inositol works as a secondary messenger in insulin signaling, making your cells more responsive to the hormone.
Women taking myo-inositol see 25-30% improvements in fasting insulin, 20-25% reductions in HOMA-IR, and restored menstrual regularity within 8 to 12 weeks. It's also safe for women trying to conceive. Stack it with magnesium and protein interventions for amplified benefits, particularly if you have PCOS or experience insulin resistance from birth control.
Consistency is crucial: myo-inositol works through cumulative cellular changes, so daily dosing for at least three months is necessary for meaningful metabolic improvement. The investment pays off with measurable changes in your lab values and symptoms.
Menstrual blood loss makes iron deficiency the most common nutrient deficiency in women aged 20-39. Ferritin shows your iron stores: optimal levels are 50 to 150 ng/mL. Below 30, your thyroid slows down and mitochondria struggle to produce energy, leading to fatigue, poor exercise recovery, and worsened insulin resistance. Women with low ferritin often experience brain fog and mood swings that don't improve with sleep or caffeine.
The most effective intervention is iron bisglycinate, which absorbs 2-3 times better than standard iron salts. Take 25 to 50 mg every other day—this approach increases absorption by 40% compared to daily dosing while reducing digestive side effects by 60%. Raising ferritin takes patience, typically requiring 3 to 6 months of consistent supplementation. Take vitamin C with iron to boost absorption, but separate magnesium by at least 2 hours to avoid competition.
Iron status affects every metabolic marker: low ferritin increases inflammation (hs-CRP), worsens insulin resistance, and undermines benefits from exercise and other supplements. Before pushing harder with workouts or tweaking your diet, check and correct iron deficiency. Once optimized, you're primed to build muscle—your body's most powerful metabolic engine.
Insulin resistance and metabolic dysfunction rarely announce themselves with dramatic symptoms in young women. Instead, they often show up as subtle, everyday issues: skin tags, darkening of skin folds (acanthosis nigricans), intense sugar cravings, and irregular or missed periods. Rapid weight changes in either direction, persistent fatigue despite adequate sleep, and mood crashes that worsen premenstrually are all red flags.
If you are on hormonal birth control, it is especially important to request fasting insulin alongside your regular bloodwork. The pill can artificially normalize glucose readings while insulin quietly climbs, masking early dysfunction. For women with PCOS or a family history of diabetes, these signs should prompt immediate investigation with the biomarkers discussed earlier.
Catching these warning signs early allows you to intervene before metabolic changes become entrenched. The next step is to integrate and personalize your supplement, nutrition, and training protocol to your unique needs and laboratory trends.
Each intervention—protein at breakfast, magnesium, inositol, iron, and resistance training—works best when matched to your specific biomarker profile, symptoms, and personal context. For example, women with PCOS may benefit most from myo-inositol and protein, while those with low ferritin should correct iron first before pushing harder with exercise. Stacking interventions amplifies results: protein plus resistance training builds muscle and blunts blood sugar swings, while magnesium and iron together support mitochondrial energy production but should be timed to avoid absorption competition.
Dose matters: 30 to 40 grams of protein at breakfast, 300 to 400 milligrams of magnesium glycinate nightly, 2 to 4 grams of myo-inositol daily, and 25 to 50 milligrams of iron bisglycinate every other day. Demographics shape every decision—reproductive age, cycle phase, birth control use, and history of under-eating all change your optimal protocol.
Tracking your biomarkers every 3 to 6 months, adjusting your stack accordingly, and watching for early warning signs creates a feedback loop for lifelong metabolic resilience. In the final section, we will summarize the strategy and look ahead to how metabolic literacy can future-proof your health.
The foundation you lay in your 20s and 30s shapes your metabolic trajectory for decades. Women who invest in understanding and optimizing their biomarkers now are much more likely to sidestep the cascade of chronic diseases that begin with quiet insulin resistance. By reframing metabolism as a hormonal, not just caloric, ecosystem, you unlock powerful tools for energy, mood, and long-term health.
The most important step is to start tracking the right biomarkers: fasting insulin, HbA1c, HOMA-IR, ferritin, hs-CRP, and triglyceride-to-HDL ratio. Layer in targeted interventions—protein at breakfast, magnesium, myo-inositol if needed, iron correction, and regular resistance training. Watch for early warning signs and personalize your approach to your unique biology.
Metabolic health is not one-size-fits-all. The sooner you become fluent in your own lab trends and symptom patterns, the more agency you gain over your future. This is not about restriction or perfection. It is about listening to your body’s real signals and building a strategy that evolves with you.
Metabolic Health in Women 18-39: Beyond Calories, Into Hormones
A Comprehensive Guide to Tracking, Optimizing, and Understanding Your Metabolism in Your Reproductive Years
Diagram glossary
- bisglycinate:
- A highly absorbable compound formed by binding a mineral to two glycine molecules.
- BMI:
- A measure of body fat based on a person's weight and height.
- carbohydrate:
- A macronutrient composed of carbon, hydrogen, and oxygen that provides energy.
- CRP:
- A blood protein that increases in response to inflammation in the body.
- Ferritin:
- A blood protein that stores iron and releases it in a controlled fashion.
- glucose:
- A simple sugar that serves as the primary energy source for cells.
- HDL:
- A beneficial lipoprotein that removes excess cholesterol from the bloodstream.
- HOMA:
- A mathematical model used to quantify insulin resistance and beta-cell function.
- Insulin:
- A hormone produced by the pancreas that regulates blood sugar levels.
- PCOS:
- A common hormonal disorder causing enlarged ovaries with small cysts.
Conclusions
Your metabolism is a dynamic hormonal ecosystem, not a simple calorie equation. For women in their reproductive years, tracking and optimizing key biomarkers—fasting insulin, HOMA-IR, HbA1c, ferritin, hs-CRP, and triglyceride-to-HDL ratio—provides actionable insights that standard advice misses. Targeted interventions such as prioritizing protein at breakfast, supplementing with magnesium glycinate, using myo-inositol for PCOS, correcting iron deficiency, and building muscle through resistance training can move these markers in real time. Personalized stacks, adjusted for your unique biology, offer the best path to lasting metabolic health and reduced chronic disease risk.
This guide is based on current clinical understanding and available evidence but does not replace individualized medical advice. The research base is still growing, especially regarding demographic nuances in women’s metabolic health. Not all interventions will work equally for every woman, and some may require professional supervision, especially with supplementation and treating iron deficiency. Laboratory ranges and optimal values may differ by assay or clinical context. Further research is needed to clarify long-term outcomes of these strategies in diverse populations.
Track this in your stack
See how berberine relates to your health goals and monitor changes in your biomarkers over time.
Sources (9)
This article informs how supplementation moves 2 markers.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.
3-month average blood glucose. Levels >= 5.7% associated with cognitive decline independent of diabetes diagnosis.
Apolipoprotein B — particle count of atherogenic lipoproteins. Levels > 80 mg/dL associated with cardiovascular event risk independent of LDL-C.