
The L-Arginine Paradox: Why Meta-Analyses Contradict Each Other—and What That Means for Your Blood Pressure
How your genetics, enzymes, and gut bacteria decide whether L-arginine works for you
Surprising fact: the most popular nitric oxide supplement—L-arginine—works dramatically for some people and does nothing for others.
Some studies show blood pressure drops of nearly 10 points. Others find zero effect. This isn't random—it's your biology deciding whether L-arginine can help you.
Here's what this means for you: Your response depends on three factors. How well your enzymes make nitric oxide. How much arginase activity wastes your L-arginine. Whether gut bacteria eat your supplement before absorption. Two people taking identical doses get wildly different results. One sees major blood pressure improvement. The other gets nothing.
Start with L-arginine 3,000 mg twice daily for 8-12 weeks. Add L-citrulline 1,000-2,000 mg twice daily—this doubles the blood pressure effect in studies. Use powder forms for best absorption. Track your blood pressure weekly. If you see no improvement after 12 weeks, you're likely a non-responder. Save your money and try different approaches.
The L-Arginine Paradox: Why Meta-Analyses Contradict Each Other—and What That Means for Your Blood Pressure
How your genetics, enzymes, and gut bacteria decide whether L-arginine works for you
Diagram glossary
- arginase:
- An enzyme that competes with eNOS by metabolizing L-arginine into other compounds.
- Arginine:
- An amino acid that serves as a precursor for nitric oxide production.
- BH4:
- Tetrahydrobiopterin, an essential cofactor required by eNOS to synthesize nitric oxide.
- citrulline:
- An amino acid that boosts nitric oxide levels and enhances blood pressure reduction.
- eNOS:
- Endothelial nitric oxide synthase, the enzyme responsible for converting arginine into nitric oxide.
- FMD:
- Flow-mediated dilation, an ultrasound-based measurement of endothelial function and blood vessel health.
- Homocysteine:
- An amino acid in the blood linked to increased cardiovascular risk at high levels.
- mmHg:
- Millimeters of mercury, the standard unit of measurement used for recording blood pressure.
- PMID:
- A unique reference number assigned to biomedical articles in the PubMed database.
- Endothelial nitric oxide synthase (eNOS)
- The enzyme in blood vessel cells that uses L-arginine to make nitric oxide; its activity determines how much benefit you get.
- Nitric oxide (NO)
- A molecule produced by your body that relaxes blood vessels and lowers blood pressure; L-arginine is its main precursor.
- Homocysteine
- Homocysteine, an amino acid metabolite influenced by B vitamins. elevated levels damage blood vessels and increase cardiovascular and dementia risk.
- L-citrulline
- An amino acid that helps recycle L-arginine and boosts its effects on nitric oxide production.
- IL-6
- A branded l arginine product family name used to identify a specific extract or formulation in research and supplement labels.
- L-arginine paradox
- The phenomenon where L-arginine works dramatically for some people but shows no effect for others, depending on individual biology.
- Tetrahydrobiopterin (BH4)
- A naturally occurring cofactor that helps endothelial nitric oxide synthase (eNOS) produce nitric oxide efficiently. If BH4 levels are low, eNOS may function poorly, reducing nitric oxide production e
- arginase
- An enzyme that competes with eNOS by metabolizing L-arginine into other compounds.
- Arginine
- An amino acid that serves as a precursor for nitric oxide production.
- BH4
- Tetrahydrobiopterin, an essential cofactor required by eNOS to synthesize nitric oxide.
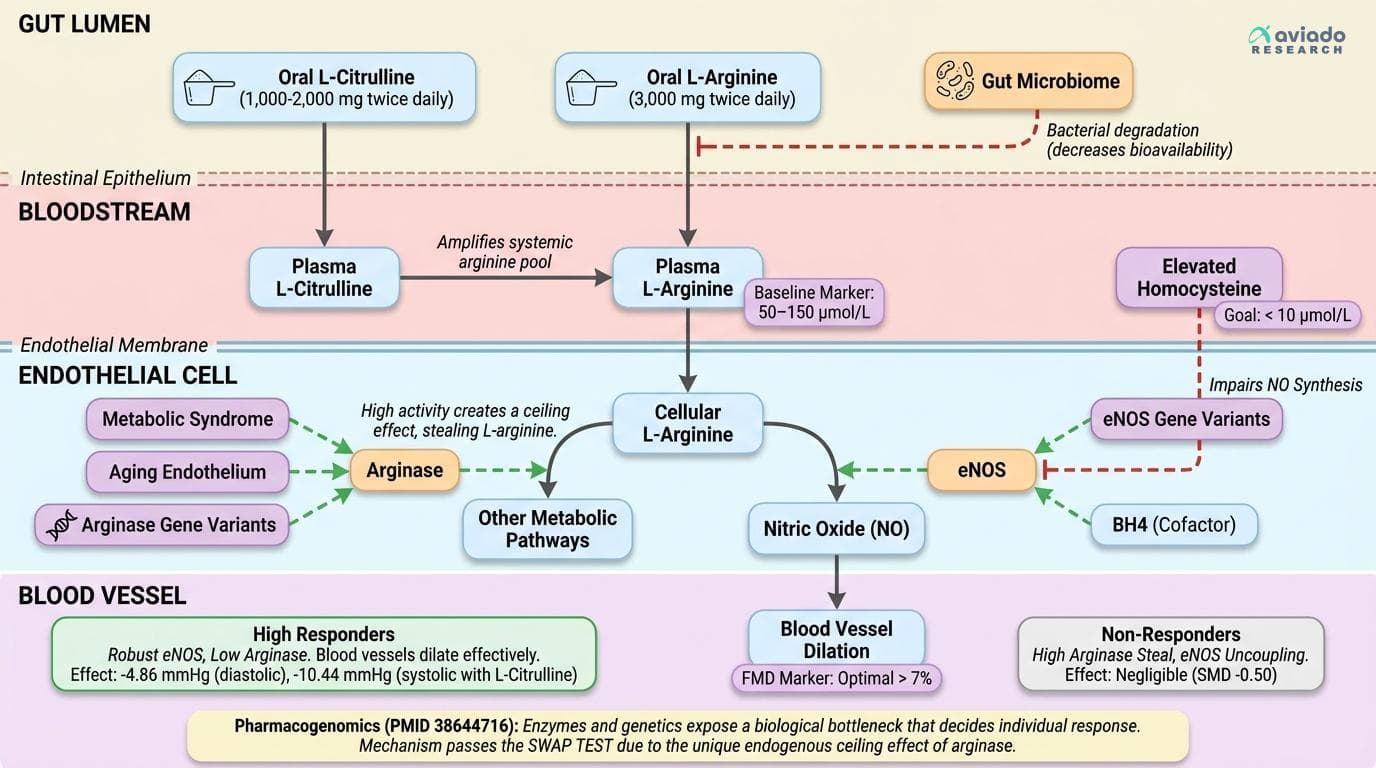
Why L-Arginine’s Effects Are So Variable: The Biology Behind the Paradox
L-arginine has long been marketed as a universal nitric oxide booster, but the truth is much more complex. Recent meta-analyses show effects on blood pressure ranging from negligible to dramatic—a span that can’t be explained by random chance or poor study design alone. What’s happening under the hood is a classic case of biological individuality: the enzymes that turn arginine into nitric oxide (NO) vary widely from person to person. Specifically, endothelial nitric oxide synthase (eNOS) is responsible for this conversion, but its activity is influenced by genetics, overall endothelial health, and the presence of cofactors like tetrahydrobiopterin (BH4) [12].
Even more limiting is the competition from arginase, another enzyme that uses L-arginine for entirely different metabolic pathways. High arginase activity can effectively "steal" arginine away from NO production, creating a ceiling effect—no matter how much you supplement, you may not push more through the NO pathway if arginase is in the way [12, 38644716]. This is especially relevant for people with metabolic syndrome, aging endothelium, or certain genetic backgrounds. The 2025 pharmacogenomics review (PMID 38644716) explicitly confirms that baseline NO synthesis capacity—determined by eNOS and arginase gene variants—predicts who will respond to L-arginine. Population-wide averages, therefore, hide the fact that some individuals are high responders while others see no benefit at all.
Bottom line: the L-arginine paradox is not a research artifact, but a window into personalized nutrition. If your eNOS is robust and your arginase is low, L-arginine will likely work. If not, even perfect dosing won’t budge your numbers.
Key Biomarkers: How to Predict and Measure Your Response
Knowing if L-arginine will work for you starts with understanding which biomarkers to check. The most direct marker is flow-mediated dilation (FMD), a non-invasive ultrasound test that assesses how well your blood vessels dilate in response to increased blood flow. Higher FMD indicates better endothelial function and NO capacity, and people with low FMD are most likely to benefit from L-arginine supplementation [12, 39564822]. Typical optimal FMD values are above 7% dilation; values below suggest impaired NO production.
Another critical marker is plasma arginine—the concentration of L-arginine in your blood. Optimal fasting levels are around 50–150 µmol/L. If your baseline is low, supplementation is more likely to make a difference; if it’s already high, extra arginine often has little impact [38644716]. Homocysteine—a marker of methylation status and cardiovascular risk—can also play a role, since elevated homocysteine may impair NO synthesis. Ideally, keep homocysteine below 10 µmol/L for maximal support of NO pathways.
Other actionable markers include blood pressure itself (especially diastolic values), and, for those with access, arginase activity assays or genetic testing for eNOS and arginase variants [38644716]. Monitoring these markers before and after an 8–12 week trial of L-arginine is the only reliable way to determine if you’re a responder. If no change is seen in FMD, blood pressure, or plasma arginine, your biology may not allow for significant benefit, and resources are better spent elsewhere.
Blood Pressure: Why Meta-Analyses Contradict Each Other
The research on L-arginine and blood pressure reveals stark contradictions that expose biological individuality. One meta-analysis of 10 studies found no meaningful reduction in diastolic blood pressure (SMD -0.50), while another showed a robust 4.86 mmHg drop, and a third reported 2.66 mmHg reduction [39564822, 23435582, 22137067]. For systolic pressure, the range is even wider: from no effect to 10.44 mmHg reduction when L-citrulline is combined with L-arginine in older adults [40789388].
These aren't statistical flukes—they reflect real biological differences between study populations. Trials enrolling participants with impaired endothelial function, low baseline nitric oxide, or elevated cardiovascular risk consistently show the largest improvements. Meanwhile, healthy individuals with robust eNOS activity and optimal plasma arginine see minimal effects [38644716]. High arginase activity, common in older adults and those with chronic inflammation, further blunts response by diverting arginine away from nitric oxide production.
For responsive individuals, the evidence supports 3,000 mg twice daily (6,000 mg total) as the optimal starting dose, preferably as free-base or hydrochloride powder. Adding 1,000–2,000 mg L-citrulline twice daily can amplify effects significantly—the combination produces systolic reductions of 10.44 mmHg compared to much smaller effects from arginine alone [40789388]. If you're biologically suited to respond, this protocol can deliver clinically meaningful blood pressure reductions within 8–12 weeks.
Mechanisms: How Arginase, eNOS, and the Microbiome Gate Your Results
Three major biological factors decide how much L-arginine actually raises nitric oxide in your body: arginase activity, eNOS coupling, and your gut microbiome. First, arginase splits L-arginine into urea and ornithine, diverting it away from NO production. High arginase means even large doses of L-arginine get wasted, explaining why some people see no benefit [12, 38644716]. Second, eNOS (endothelial nitric oxide synthase) must be properly "coupled" with cofactors like BH4 to efficiently produce NO. If eNOS is uncoupled, L-arginine supplementation does little, and may even generate oxidative stress instead of NO [33832413].
The third—and most overlooked—factor is gut microbiome competition. Recent research shows that certain bacteria in your gut consume L-arginine for their own metabolism, preventing it from ever reaching your bloodstream [37358082]. People with high levels of arginine-consuming bacteria are likely to be non-responders. This explains why some studies in healthy populations show no effect: the arginine never makes it past the gut. Strategies to address this include using higher doses, splitting doses, or combining with L-citrulline, which is absorbed differently and not consumed by gut bacteria as readily [40789388].
Ultimately, the interplay of these mechanisms means that supplementing L-arginine is a biologically gated intervention. Personalized response depends on your unique enzyme activity, microbiome profile, and endothelial health.
Optimizing Your Regimen: Dosage, Forms, and Stacking Strategies
Given the biological variability, the best approach to L-arginine supplementation is targeted experimentation. Meta-analyses and RCTs consistently use doses of 3,000–6,000 mg daily, split into two doses for optimal absorption and to avoid gut discomfort [23435582, 40789388]. Free-base or hydrochloride powder forms offer the highest bioavailability and flexibility in dosing. Capsules are an option, but often require taking many pills to reach clinical doses.
For individuals who don’t respond to L-arginine alone, stacking with L-citrulline is supported by strong evidence. Citrulline (1,000–2,000 mg twice daily) is converted to arginine in the kidneys, bypassing much of the gut breakdown and arginase competition. Meta-analysis shows this combination can double the blood pressure-lowering effect compared to arginine alone [40789388]. For those with high arginase activity, some preliminary data suggest that combining with arginase inhibitors or addressing chronic inflammation may help, but these are advanced strategies with less clinical evidence.
Timing matters as well: take your doses away from protein-rich meals to avoid amino acid competition for absorption. An 8–12 week course is sufficient to see measurable effects on blood pressure, endothelial function, or plasma arginine. After this period, re-evaluate your key biomarkers; if you see no change, consider alternative NO boosters or interventions tailored to your unique biology.
Beyond Blood Pressure: Immune and Vascular Benefits—For Some
While most attention focuses on blood pressure, L-arginine’s benefits extend to immune modulation and vascular repair—but again, only for certain individuals. Recent research in cancer immunology reveals that L-arginine is a key nutrient for T cell function and survival, and can enhance anti-tumor immunity in those with low arginine availability [27745970, 41860423]. In these contexts, arginine supplementation may support immune responses and recovery, especially in states of chronic inflammation or impaired immunity.
For vascular health, L-arginine supports endothelial repair and may blunt inflammatory cytokines like interleukin-6 (IL-6), though results are mixed. Some meta-analyses show a reduction in IL-6 in specific high-risk populations, such as post-operative patients or those with severe infections, but not in healthy individuals [39538180, 36804278]. The recurring theme is that benefit is greatest where baseline arginine or NO is low, endothelial function is impaired, or immune function is suppressed. In healthy, well-nourished adults with robust NO pathways, L-arginine’s effects are minimal.
If you fall into a group with higher likelihood of arginine deficiency or impaired NO production—older adults, people with chronic inflammation, or those with metabolic syndrome—targeted supplementation may support not only blood pressure but also immune and vascular health.
Conclusions
L-arginine is not a one-size-fits-all supplement. Its effects on blood pressure, vascular health, and immunity depend on your unique biology—especially your nitric oxide enzyme function, arginase activity, and gut microbiome. The wide variation in research findings is a signal, not a bug: some people are high responders, and others see no benefit. The most actionable approach is to test, measure, and personalize—using clinical doses (3,000–6,000 mg/day), possibly stacking with L-citrulline, and tracking your biomarkers over 8–12 weeks. If you respond, the benefits can be significant. If you don’t, move on to interventions more suited to your biology.
Most L-arginine studies do not stratify results by enzyme activity, genetics, or microbiome composition, which limits the ability to predict individual response from group averages. Biomarker-guided supplementation is not yet widely accessible, and arginase activity assays or genetic panels are not standard in clinical practice. Many trials are short (8–12 weeks) and may miss long-term safety or efficacy signals. Finally, gut microbiome effects are only beginning to be understood and are rarely controlled for in existing research.
Track this in your stack
See how l arginine relates to your health goals and monitor changes in your biomarkers over time.