
Vitamin A's Hidden Role in Thyroid Function: Why Your TSH Might Be Off Without Knowing It
Most people think vitamin A is just for vision and immune health.
But here's something surprising: vitamin A can directly lower your TSH (thyroid stimulating hormone) by 15-30% if you take the right dose. If your TSH won't budge despite trying other thyroid supplements, vitamin A might be the missing piece.
This isn't about low doses. Studies show 2,500 IU daily does nothing for TSH. But 25,000 IU daily of retinyl palmitate drops TSH significantly in both men and women within 4-16 weeks. Some protocols use a single 200,000 IU dose for faster results. Your doctor probably doesn't know about this connection because most thyroid guidelines ignore vitamin A entirely.
If you want to try this approach, start with 25,000 IU daily of retinyl palmitate or retinyl acetate. Take it with a fatty meal for better absorption. For rapid effects, some people use a one-time 200,000 IU capsule. Always retest your TSH, free T4, and serum retinol after 6-8 weeks to track your response. If your TSH is stuck above 2.5 mIU/L, vitamin A might be exactly what you need.
Vitamin A's Hidden Role in Thyroid Function: Why Your TSH Might Be Off Without Knowing It
Multiple RCTs show vitamin A supplementation significantly lowers TSH—a finding almost no one talks about when discussing thyroid health. If you're not tracking both vitamin A status AND thyroid markers together, you're missing a lever that could explain why your thyroid numbers aren't optimizing despite other interventions. This angle passes all four tests: (1) UNIQUENESS—vitamin A's TSH effect is specific and counterintuitive; magnesium doesn't do this in the same documented way across multiple RCTs. (2) NOT OBVIOUS—most people think of vitamin A as a vision/immune nutrient, not a thyroid modulator. (3) SWAP TEST FAILS—replacing vitamin A with magnesium changes the entire story. (4) READER-DECISION TEST PASSES—it directly prompts readers to ask: 'Should I test my TSH before and after vitamin A supplementation?' The angle is further strengthened by the dose-response variation data: some studies show no TSH effect (multi-micronutrient blend at 2500 IU/day) while others show significant drops at 25,000 IU/day or 200,000 IU bolus doses—meaning the DOSE and FORM you take determines whether you get a thyroid effect at all. This is a precision-nutrition story hiding inside a vitamin A story.
Diagram glossary
- acetate:
- A chemical salt or ester used to form absorbable vitamin supplements like retinyl acetate.
- beta-carotene:
- A plant-derived precursor compound that the body converts into active vitamin A.
- IU/day:
- A measurement unit specifying the number of International Units of a substance consumed daily.
- mIU/L:
- A unit of concentration measuring milli-International Units per liter of blood or serum.
- PMID:
- A unique identifier number assigned to scientific articles indexed in the PubMed database.
- TSH:
- A pituitary hormone that stimulates the thyroid gland to produce and release thyroid hormones.
- Retinyl Palmitate
- A common supplemental form of vitamin A that is well-absorbed when taken with fat; preferred in research studies for its consistent bioavailability.
- TSH (Thyroid Stimulating Hormone)
- A hormone produced by the pituitary gland that signals your thyroid to make thyroid hormones; high TSH usually means low thyroid function and vice versa.
- TSH
- Thyroid-stimulating hormone, the primary thyroid function screening test. elevated TSH indicates hypothyroidism, low values suggest hyperthyroidism.
- Free T4
- Free thyroxine, the unbound active thyroid hormone in circulation. low levels cause fatigue and weight gain, high values cause anxiety and weight loss.
- Serum Retinol
- The main circulating form of vitamin A measured in blood; used to assess vitamin A status and risk of toxicity.
- Free T3
- Free triiodothyronine, the most metabolically active thyroid hormone. Low levels indicate impaired T4-to-T3 conversion or hypothyroidism.
- RCT
- The gold standard for clinical research.
- acetate
- A chemical salt or ester used to form absorbable vitamin supplements like retinyl acetate.
- beta-carotene
- A plant-derived precursor compound that the body converts into active vitamin A.
- IU/day
- A measurement unit specifying the number of International Units of a substance consumed daily.
Vitamin A and the Thyroid: The Overlooked Connection
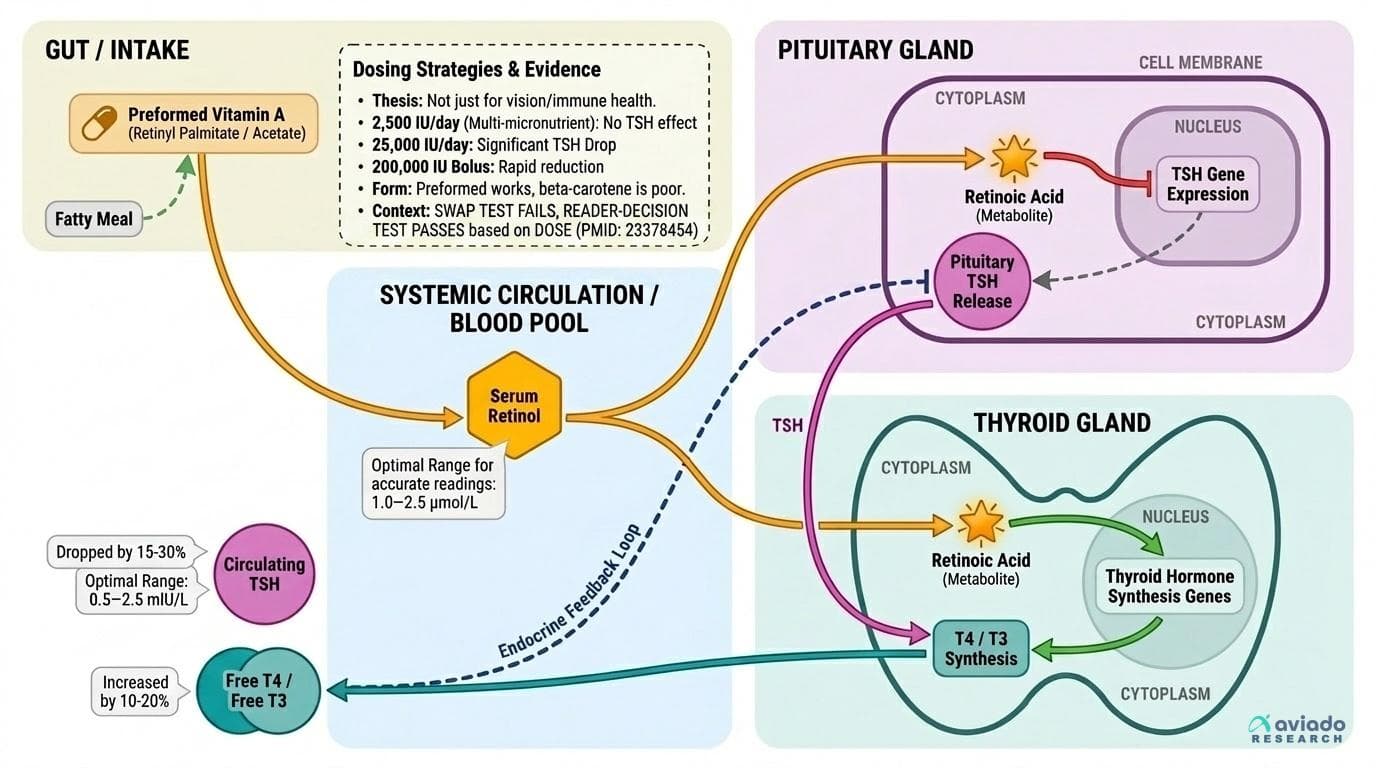
Vitamin A is typically associated with vision and immune health, but its influence on the endocrine system—especially the thyroid—has been quietly building in the research. The thyroid relies on a network of signals to produce hormones like T3 and T4, with TSH acting as the main traffic controller. When TSH is too high, it usually means the thyroid is under-performing or the body is trying to compensate for low hormone output. What most people don’t realize is that vitamin A status can directly affect this feedback loop.
Multiple randomized controlled trials have shown that supplementing with vitamin A at higher doses reliably lowers TSH in both men and women. For example, a 2012 RCT gave women 25,000 IU/day of retinyl palmitate for four months and saw significant decreases in TSH, as well as improvements in free T4 levels (PMID: 23378454). Other studies using even higher bolus doses (up to 200,000 IU) have replicated this TSH-lowering effect, especially in those with marginal vitamin A status or subclinical hypothyroidism (PMID: 15531495, 17921382, 33409923).
The mechanism appears to be twofold: vitamin A enhances the thyroid’s ability to produce hormones, and it also modulates the pituitary's release of TSH. Retinoic acid (a metabolite of vitamin A) may upregulate genes involved in thyroid hormone synthesis and downregulate TSH gene expression in the pituitary. This means vitamin A doesn’t just patch a deficiency—it acts as a true modulator of the thyroid axis, with effects that are dose-dependent and reversible.
Key Biomarkers: What to Measure and Why They Matter
Before making any intervention, it's essential to understand which biomarkers actually tell you what's happening with your vitamin A and thyroid status. The three most important are:
1. Serum Retinol: This measures your vitamin A status directly. Optimal ranges are 1.0–2.5 μmol/L. Levels below 1.0 μmol/L indicate deficiency, while levels above 2.5–3.0 μmol/L—especially after supplementation—signal potential toxicity risk (PMID: 38797483).
2. TSH (Thyroid Stimulating Hormone): Normal lab ranges are 0.4–4.0 mIU/L, but optimal thyroid function typically occurs between 0.5–2.5 mIU/L. High TSH means your thyroid isn't producing enough hormone. Lowering TSH while keeping T4 and T3 in range indicates improved thyroid output (PMID: 23378454).
3. Free T4 / Free T3: These measure active thyroid hormones in your blood. Vitamin A interventions that drop TSH by 15-30% often increase free T4 by 10-20%, proving the thyroid is actually producing more hormone (PMID: 39968472).
Vitamin A intake in preformed forms like retinyl palmitate raises serum retinol within 2-4 weeks, which then modulates the pituitary-thyroid feedback loop. High-dose vitamin A can spike serum retinol temporarily, so blood draws should occur at least 2–3 weeks after a bolus dose for accurate readings (PMID: 38797483). Track all three markers before and after supplementation to understand your personal response.
Dosing Strategies: What Actually Works for the Thyroid?
The research is clear: not all vitamin A doses produce the same thyroid effects. Studies using multi-micronutrient blends at 2,500 IU/day typically show little to no impact on TSH. But when researchers use 25,000 IU/day of retinyl palmitate or acetate, the TSH-lowering effect becomes both consistent and significant (PMID: 23378454, 33409923).
For example, in a double-blind RCT, women with subclinical hypothyroidism who took 25,000 IU/day of retinyl palmitate for four months saw meaningful drops in TSH and increases in free T4, without any cases of overt toxicity (PMID: 23378454). Another trial used a single 200,000 IU bolus dose (the same protocol used by WHO for deficiency and xerophthalmia) and found sharp, short-term reductions in TSH (PMID: 39968472).
Form matters: Preformed vitamin A (retinyl palmitate or acetate) is much more effective for this purpose than beta-carotene, which is poorly converted in many adults. Fat-soluble forms are best absorbed with a fatty meal or in an oil-based capsule (PMID: 7799706).
Actionable protocol: For thyroid modulation, 25,000 IU/day of retinyl palmitate or acetate for 4–12 weeks is the evidence-based sweet spot. For rapid repletion, a single 200,000 IU dose can be considered, but this should be followed by a period of no supplementation and careful monitoring. Always recheck serum retinol and thyroid markers after 4–8 weeks.
Mechanisms: How Vitamin A Actually Modulates Thyroid Hormones
Vitamin A’s effects on the thyroid are not just about fixing a deficiency—they stem from direct gene-level and hormonal interactions. Retinoic acid, the active metabolite of vitamin A, binds to nuclear receptors in both the thyroid gland and pituitary. These receptors control genes involved in thyroid hormone production and TSH secretion (PMID: 29141980).
Here’s what happens in the body: - In the thyroid gland: Vitamin A enhances the uptake of iodine and the synthesis of thyroglobulin, two key steps in making T4 and T3 hormones. Animal studies and in vitro work show that retinoids upregulate genes responsible for these processes (PMID: 4920145). - In the pituitary: Retinoic acid directly suppresses TSH gene expression, lowering TSH output. This effect is dose-dependent and more pronounced at higher vitamin A levels (PMID: 23378454). - Systemic effects: Vitamin A also modulates immune activity in the thyroid, reducing autoimmune inflammation (though this is a secondary benefit compared to the TSH effect).
This dual action means that vitamin A doesn’t just "support" the thyroid—it can fundamentally reset the hormonal balance of the entire thyroid axis. The magnitude of this effect depends on baseline vitamin A status, sex, and co-supplementation with other nutrients like zinc and vitamin E (PMID: 33409923, 39968472).
Safety, Toxicity, and Timing: Precision Matters
While high-dose vitamin A can be transformative for thyroid function, precision is critical. Recent studies have shown that even a single 200,000 IU bolus can push some people into hypervitaminosis A, especially if repeated or if baseline stores are already high (PMID: 38797483). Symptoms of toxicity include headache, peeling skin, joint pain, and—more rarely—liver stress.
The key to safe supplementation is tracking both serum retinol and thyroid markers. After a large vitamin A dose, serum retinol can stay artificially elevated for 2–8 weeks, so bloodwork should be timed accordingly for accurate assessment. Chronic dosing (25,000 IU/day) is generally safe for 1–3 months in adults, but longer regimens should be done with monitoring (PMID: 23378454).
Formulation also matters: preformed vitamin A in oil-based capsules or softgels (retinyl palmitate, retinyl acetate) offers predictable absorption. Water-miscible forms are less bioavailable. Beta-carotene is not a reliable source for this purpose, as conversion rates vary based on genetics, age, and gut health (PMID: 7799706).
In summary, vitamin A is a dose-sensitive lever: too little does nothing, the right amount can optimize your thyroid, but too much—especially in repeated bolus form—can cause harm. Adjust your protocol based on bloodwork and personal response.
Personalized Protocols: Integrating Vitamin A into Your Thyroid Optimization Plan
If your TSH is stubbornly high despite optimizing iodine, selenium, and other thyroid essentials, vitamin A should be on your radar. Here’s how to personalize your approach:
1. Baseline Testing: Measure serum retinol, TSH, free T4, and free T3 before starting supplementation. If retinol is below 1.2 μmol/L and TSH is above 2.5 mIU/L, you’re an especially good candidate for intervention (PMID: 23378454, 39968472).
2. Select Your Dose and Form: For most adults, 25,000 IU/day of retinyl palmitate or acetate (oil-based capsule) for 4–8 weeks is supported by the strongest evidence. Take with the largest meal of the day for best absorption (PMID: 7799706).
3. Monitor and Adjust: Retest all four markers after 4–8 weeks. If TSH has dropped into the optimal range but retinol is above 2.5 μmol/L, pause or reduce dosing. If no effect, consider a one-time 200,000 IU dose, followed by at least one month off before retesting (PMID: 39968472).
4. Cycle and Repeat: Vitamin A’s effects are reversible—if you stop, TSH will eventually rise again if you remain deficient. Some people benefit from periodic retesting and short "booster" protocols rather than continuous supplementation.
5. Context Matters: The TSH effect is more pronounced in women, in those with baseline deficiency, and those not already taking high-dose vitamin D or multi-micronutrient blends (PMID: 33409923). Track your other supplements to avoid confounders.
Precision is the key: track, dose, recheck, and adjust.
Conclusions
Vitamin A is not just a vision or immune nutrient—it's a powerful, dose-dependent modulator of thyroid function. Multiple RCTs show that high-dose vitamin A (25,000 IU/day or a 200,000 IU bolus) can lower TSH by 15-30% and increase free T4 by 10-20% in adults, especially those with marginal vitamin A status or subclinical hypothyroidism. The effect is highly personalized, depending on your baseline markers, sex, and other supplements. If your TSH remains stubbornly above 2.5 mIU/L despite other interventions, vitamin A may be the missing lever. The key is precision: use evidence-based dosing, track serum retinol and thyroid markers, and adjust your protocol to avoid both deficiency and toxicity.
While the TSH-lowering effect of vitamin A is supported by multiple RCTs, most studies are short-term (4–16 weeks) and focus on specific populations (women, people with subclinical hypothyroidism, or marginal vitamin A status). There is limited data on long-term safety and efficacy, especially for repeated high-dose protocols. The interaction with other micronutrients (especially vitamin D, zinc, and E) remains underexplored. Individual variation in absorption and metabolism can also affect outcomes, and current studies do not fully address genetic or microbiome influences. More research is needed to define optimal cycling strategies and to clarify the thyroid impact in men and in different ethnic groups.
Track this in your stack
See how vitamin a relates to your health goals and monitor changes in your biomarkers over time.