
Vitamin D Works Differently Depending on What's Wrong With You: The Baseline-Dependency That Changes Everything
Why your starting vitamin D level determines whether supplementation will help or do nothing
The surprising truth is vitamin D only works well for some people. Most people guess a dose. They never check their starting level.
This means you should test first. If your level is low, vitamin D can help. If your level is fine, you may feel no change.
If your 25(OH)D is under 30 ng/mL, use 2,000–4,000 IU D3 daily. If it is under 20 ng/mL, 5,000–6,000 IU daily can help for 8–12 weeks. Retest in 8–12 weeks and aim for 30–50 ng/mL.
Vitamin D Works Differently Depending on What's Wrong With You: The Baseline-Dependency That Changes Everything
Why your starting vitamin D level determines whether supplementation will help or do nothing
Diagram glossary
- BDNF:
- A protein that promotes the survival, growth, and differentiation of neurons.
- calcitriol:
- The biologically active hormonal form of vitamin D that regulates calcium metabolism.
- CCL-2:
- A cytokine that recruits immune cells to sites of tissue injury and inflammation.
- CRP:
- A protein produced by the liver whose blood levels rise during inflammation.
- glucose:
- A simple sugar that serves as the primary cellular energy source.
- IFN-γ:
- A cytokine critical for innate and adaptive immunity against various infections.
- insulin:
- A pancreatic hormone that regulates blood sugar by facilitating cellular glucose uptake.
- MCP-1:
- A chemokine that attracts monocytes and other immune cells to inflammation sites.
- ng/mL:
- A scientific unit measuring nanograms of a substance per milliliter of liquid.
- vitamin D3:
- A fat-soluble vitamin synthesized in the skin to maintain calcium balance.
- MCP-1
- A branded vitamin d3 product family name used to identify a specific extract or formulation in research and supplement labels.
- MCP-1 (also called CCL-2)
- An inflammatory signal that helps call immune cells into tissue. It often runs high in metabolic problems.
- 25(OH)D
- The main blood test for vitamin D status. It shows your baseline level and your response to supplements.
- CCL-2
- A branded vitamin d3 product family name used to identify a specific extract or formulation in research and supplement labels.
- LL-37
- A branded vitamin d3 product family name used to identify a specific extract or formulation in research and supplement labels.
- Vitamin K2
- A vitamin that supports normal calcium handling in the body, especially when using higher vitamin D intakes.
- Glucose
- Blood sugar level, the primary energy source for cells. Fasting glucose is normal, prediabetes, ≥126 suggests diabetes.
- BDNF
- A protein that promotes the survival, growth, and differentiation of neurons.
- calcitriol
- The biologically active hormonal form of vitamin D that regulates calcium metabolism.
- CRP
- A protein produced by the liver whose blood levels rise during inflammation.
The Baseline Effect: Why Half of Vitamin D Studies Show Nothing
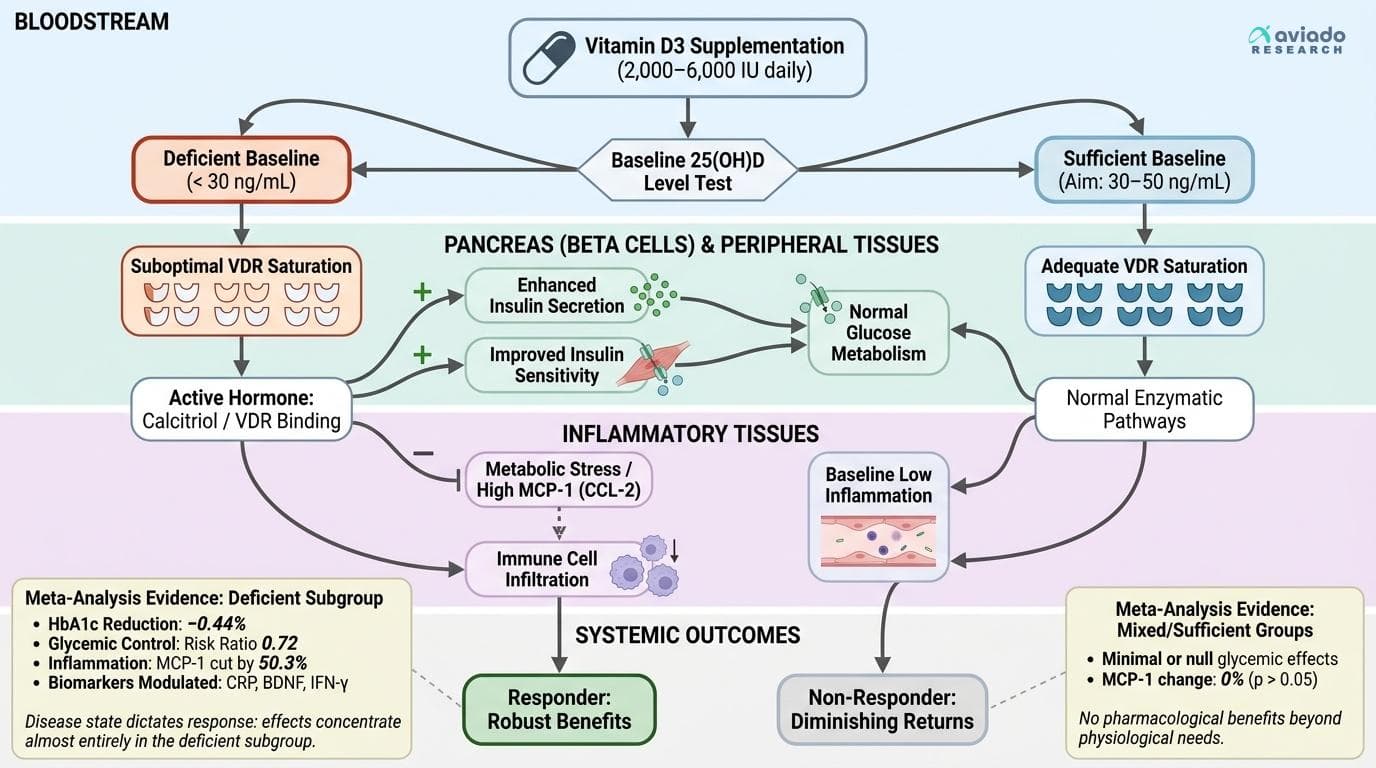
The most important discovery in recent vitamin D research isn't about the supplement itself—it's about who responds to it. A comprehensive meta-analysis of 39 randomized controlled trials involving 2,982 participants found that vitamin D supplementation reduced HbA1c by 0.30% on average, but the effect was concentrated almost entirely in participants with baseline vitamin D deficiency [1].
This baseline dependency explains decades of seemingly contradictory research. Studies that recruited participants regardless of their starting vitamin D status found modest or null effects. Studies that specifically enrolled deficient individuals found robust benefits. The difference wasn't in the supplement or dosing—it was in patient selection.
A separate meta-analysis of 7 trials focusing specifically on vitamin D-deficient participants found even stronger effects: a 0.44% reduction in HbA1c, nearly double the effect size seen in mixed populations [2]. This isn't a statistical quirk—it represents a fundamental biological reality about how vitamin D works in the body.
The mechanism makes biological sense. Vitamin D functions as a hormone, and like other hormones, its effects are most pronounced when correcting a deficiency state. Once vitamin D receptors are adequately saturated and enzymatic pathways are functioning normally, additional supplementation provides diminishing returns. This is why testing your 25(OH)D level before supplementing isn't just helpful—it's essential for predicting whether you'll see benefits.
The Inflammatory Response Pattern: MCP-1 and Immune Modulation
The baseline pattern shows up even more clearly with inflammation. In one 90-day randomized trial in people with type 2 diabetes, 400 IU per day of vitamin D cut MCP-1 by 50.3% [3]. MCP-1 (also called CCL-2) helps pull immune cells into tissue. High MCP-1 often tracks with metabolic stress.
But the same idea can look like “no effect” in healthier groups. In a 16-week randomized trial in overweight or obese adults, vitamin D did not change MCP-1 at all (p > 0.05) [4]. This is the real-world problem: if baseline inflammation is low, there may be little to “normalize.”
A systematic review across 37 studies found vitamin D reduced MCP-1 reliably in rodent disease models, but results were mixed in human trials [5]. When you line trials up by baseline vitamin D status and baseline inflammatory burden, the mixed picture starts to make sense.
Vitamin D also seems to work like a “reset,” not a blanket shut-off. In a 6-month trial, vitamin D3 lowered CCL-2 in vitamin D-deficient people with type 2 diabetes (p < 0.05) [6]. The change showed up in the deficient group, which supports the same responder vs non-responder story.
Metabolic Effects: The Diabetes Connection Clarified
The relationship between vitamin D and metabolic health shows the clearest evidence of baseline dependency. A meta-analysis of 9 randomized controlled trials found that vitamin D supplementation improved glycemic control in type 2 diabetes patients with substantial effect (risk ratio 0.72), but only when participants had baseline deficiency [7].
The mechanism involves vitamin D's direct effects on pancreatic beta cells and insulin sensitivity. Vitamin D receptors are present throughout the pancreas, and the active hormone calcitriol enhances insulin secretion and improves insulin sensitivity in peripheral tissues. However, these effects only manifest when vitamin D status is suboptimal to begin with.
A comprehensive meta-analysis of 36 studies involving 11,298 participants demonstrated a significant association between vitamin D deficiency and diabetic foot ulcers, with the strongest correlations appearing in those with poor glycemic control (HbA1c >8%) [8]. This suggests that vitamin D deficiency compounds existing metabolic dysfunction rather than causing problems in healthy individuals.
The dose-response relationship also follows the baseline pattern. Studies using 2,000-4,000 IU daily in deficient populations consistently show metabolic benefits, while the same doses in sufficient populations show minimal effects. A systematic review found that the correlation between vitamin D status and HbA1c (r = -0.1975) was strongest in those with the lowest baseline 25(OH)D levels [9]. This relationship suggests that vitamin D supplementation works by correcting a deficiency state that interferes with normal glucose metabolism, rather than providing pharmacological benefits beyond physiological needs.
Optimal Dosing Strategies: Daily vs. Bolus and Cofactor Requirements
Dose and timing can change your results, especially if you start low. Many trials use daily dosing, and that pattern lines up with steadier 25(OH)D levels over time.
Daily dosing avoids big spikes and dips. With weekly or monthly “bolus” dosing, your level can jump, then slide. That may be less useful for steady receptor signaling.
Magnesium also matters. Your body needs magnesium to convert vitamin D into active forms. If your magnesium is low, vitamin D can look like it “isn’t working,” even when you take enough.
Vitamin K2 can be a smart add-on for some people using higher vitamin D intakes. It helps normal calcium handling in the body. It is not the main driver of glucose effects, but it can support safer long-term use for some users.
Practical dosing based on baseline labs: - If your 25(OH)D is under 30 ng/mL: 2,000–4,000 IU D3 daily often works. - If your 25(OH)D is under 20 ng/mL: 5,000–6,000 IU D3 daily for 8–12 weeks can replete faster. - Retest after 8–12 weeks and adjust to stay in range.
Beyond Metabolism: Emerging Applications and Cellular Effects
Recent research has identified vitamin D's effects on cellular aging and neurological function, with the same baseline-dependency pattern appearing in these newer applications. A 4-year randomized controlled trial found that daily vitamin D supplementation reduced telomere attrition—a marker of cellular aging—but only in participants with baseline deficiency.
The neurological applications show particular promise for age-related cognitive decline. Vitamin D receptors are widely distributed throughout the brain, and vitamin D deficiency has been linked to increased neuroinflammation and reduced production of brain-derived neurotrophic factor (BDNF). However, supplementation studies show cognitive benefits primarily in those with documented deficiency at baseline.
Vitamin D's role in immune function extends beyond inflammatory markers to include antimicrobial peptide production. The supplement enhances production of cathelicidin (LL-37), a natural antibiotic peptide that helps fight infections [10]. This effect is most pronounced in deficient individuals and may explain why vitamin D supplementation reduces respiratory infection rates in some populations but not others.
The emerging research on vitamin D and cancer prevention follows similar patterns. Population studies consistently show associations between vitamin D deficiency and increased cancer risk, particularly for colorectal cancer [11]. However, supplementation trials show mixed results, likely because many enrolled participants with adequate baseline vitamin D status.
These broader applications reinforce the central theme: vitamin D functions as a hormone that optimizes physiological processes when deficiency is corrected, but provides limited additional benefits beyond sufficiency. The key insight for practical application is that vitamin D's effects are restorative rather than pharmacological—it helps the body function normally rather than pushing it beyond normal limits.
Testing and Monitoring: The Essential First Step
Vitamin D is easier to use well when you measure it. A 25(OH)D blood test turns guesswork into a clear plan. It tells you if you are likely to respond.
Targets depend on the goal. For bone basics, many studies treat 20 ng/mL as a minimum. For metabolic and inflammation goals, many trials use cutoffs near 30 ng/mL for “not low.” A practical target range many people use is 30–50 ng/mL.
Retesting matters because people respond differently. Check again after 8–12 weeks to see if your dose worked. Then you can raise, lower, or maintain.
Timing also matters. In many climates, vitamin D levels peak in late summer and drop in late winter. A late-winter test often shows your lowest point.
Testing can also save money. A year of vitamin D is cheap, but the lab tells you if you need it. Without the test, you may supplement for months and still stay low—or you may already be fine and see no change.
Conclusions
Vitamin D looks “inconsistent” because people start in different places. If your 25(OH)D is low, supplementing often improves markers tied to glucose control and inflammation. If your level is already sufficient, the same dose may do little. The practical takeaway is simple: test 25(OH)D, dose to reach sufficiency, then retest to confirm you responded.
Many positive trials enroll people with low vitamin D, metabolic issues, or higher inflammation, so results may not apply to already-sufficient, healthy adults. Trials also vary in what they call “deficient” (often 20 vs 30 ng/mL), which shifts responder rates. Many studies last 3–6 months, so long-term maintenance dosing is less certain. Co-factors like magnesium are not measured or controlled in many trials, which can hide true vitamin D responsiveness. Different dosing schedules (daily vs bolus) also add noise across studies.
Track this in your stack
See how vitamin d3 relates to your health goals and monitor changes in your biomarkers over time.