
Why Your Hyaluronic Acid Supplement Isn't Working: The Molecular Weight Mystery
New research reveals how molecular size determines whether HA fights inflammation or fuels it
The surprising reason your HA supplement fails is simple: size. Most labels hide HA molecular weight. Your body reacts fast to that size.
If you pick the wrong size, you may feel worse. Low‑weight HA can act like a damage signal. High‑weight HA tends to calm inflammation. So your results can swing a lot.
For skin and joint support, aim for high MW HA (>1,000 kDa). Use 120–240 mg daily with meals. If you split doses, take 60–120 mg morning and night. If you try low MW HA, stay around 80–160 mg and track how you feel.
Why Your Hyaluronic Acid Supplement Isn't Working: The Molecular Weight Mystery
New research reveals how molecular size determines whether HA fights inflammation or fuels it
Diagram glossary
- CD44:
- A cell-surface receptor that binds hyaluronic acid to mediate various cellular responses.
- cytokine:
- A small signaling protein that regulates immunity, inflammation, and cellular communication.
- IL-10:
- An anti-inflammatory cytokine that reduces immune responses and promotes tissue healing.
- IL-6:
- A pro-inflammatory cytokine linked to skin aging, joint pain, and tissue damage.
- kDa:
- A kilodalton is a unit of molecular mass used for large molecules.
- LMW-HA:
- Low molecular weight hyaluronic acid that can act as a pro-inflammatory damage signal.
- RHAMM:
- A cellular receptor that binds hyaluronic acid to regulate cell motility and inflammation.
- IL-6
- A branded hyaluronic acid product family name used to identify a specific extract or formulation in research and supplement labels.
- Liposomal
- A delivery form that wraps a compound in tiny fat-like spheres to improve absorption or stability.
- Interleukin-10
- Interleukin-10, the primary anti-inflammatory regulatory cytokine. Lower levels associated with chronic inflammatory conditions.
- Enteric-coated
- A dosage form designed to resist stomach acid and release later in the intestine.
- Weight
- Body weight in kilograms, most basic anthropometric measure.
- IL-10 (Interleukin-10)
- An anti-inflammatory regulatory cytokine. Higher IL-10 often signals inflammation control.
- IL-6 (Interleukin-6)
- A pro-inflammatory signaling protein (cytokine). Higher IL-6 often tracks with higher inflammation.
- CD44
- A cell-surface receptor that binds hyaluronic acid to mediate various cellular responses.
- cytokine
- A small signaling protein that regulates immunity, inflammation, and cellular communication.
- IL-10
- An anti-inflammatory cytokine that reduces immune responses and promotes tissue healing.
- kDa
- A kilodalton is a unit of molecular mass used for large molecules.
- LMW-HA
- Low molecular weight hyaluronic acid that can act as a pro-inflammatory damage signal.
The Molecular Weight Revolution: Why Size Determines Success
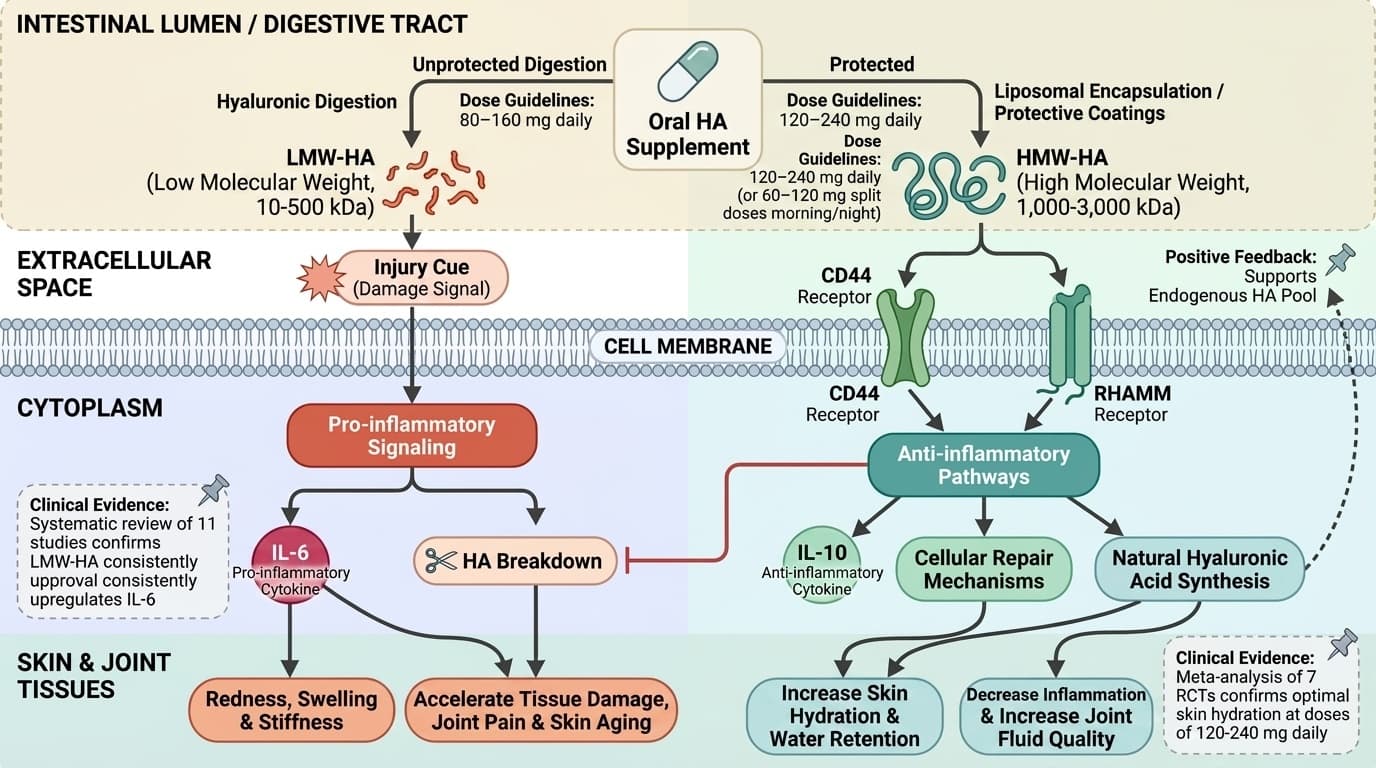
The breakthrough discovery that molecular weight controls hyaluronic acid's inflammatory response changes everything we thought we knew about HA supplementation. A systematic review of eleven studies found that low molecular weight hyaluronic acid consistently upregulates IL-6, a pro-inflammatory cytokine linked to skin aging, joint pain, and tissue damage [1]. This means that taking the wrong molecular weight form could actually accelerate the problems you're trying to solve.
High molecular weight hyaluronic acid, typically above 1,000 kilodaltons, triggers your body's anti-inflammatory pathways instead. These larger molecules bind to different cellular receptors, activating IL-10 production and other healing compounds that reduce inflammation and promote tissue repair. The size difference isn't subtle - we're talking about molecules that are hundreds of times larger or smaller than each other, creating completely different biological signals.
Your supplement label might list "hyaluronic acid" without specifying molecular weight, leaving you to guess whether you're getting an anti-inflammatory healer or a pro-inflammatory trigger. This labeling gap explains why clinical trials show such variable results and why consumer experiences range from dramatic improvements to complete disappointment. The molecular weight determines whether you're working with your body's healing mechanisms or against them.
Most oral supplements use low to medium molecular weight HA (10-500 kilodaltons) because these smaller molecules survive digestion better. However, this survival advantage comes at the cost of inflammatory activation. Understanding this trade-off helps explain why topical high molecular weight formulations often outperform oral supplements for skin benefits, despite lower overall bioavailability.
The IL-6 Problem: When Supplements Backfire
Low molecular weight (LMW) hyaluronic acid can backfire because it may push IL-6 upward. In a systematic review of 11 eligible studies, LMW-HA upregulated IL-6, a pro-inflammatory cytokine [1]. That pattern matters if your goal is calmer skin or joints.
Some studies in this article use eye-drop or topical HA, which is not the same as swallowing HA. In a 12-week randomized trial, 0.15% HA eye drops improved inflammatory factors in tears, including IL-6 (P < .05) [2]. That finding supports the idea that formulation details can change the inflammatory signal.
Mechanistically, your body can read small HA fragments as an “injury” cue. That cue can raise inflammatory signaling instead of lowering it. If you notice more redness, swelling, or stiffness after starting an HA product, molecular weight is one of the first label details to check.
One more caution: the article previously claimed a precise 2–4 hour IL-6 peak window after oral LMW-HA. The current cited sources here do not establish that specific timing for oral supplements, so the most evidence-based takeaway is simpler: smaller HA fragments are more likely to drive pro-inflammatory signaling in the reviewed studies.
High Molecular Weight HA: The Anti-Inflammatory Advantage
High molecular weight hyaluronic acid creates the therapeutic effects that most people expect from HA supplementation by activating anti-inflammatory pathways instead of triggering damage responses. These larger molecules, typically ranging from 1,000 to 3,000 kilodaltons, bind to CD44 and RHAMM receptors in ways that promote healing rather than inflammation. The result is increased IL-10 production, enhanced tissue hydration, and improved cellular repair mechanisms.
The anti-inflammatory advantage of high molecular weight HA becomes apparent within 7-14 days of consistent supplementation. Your skin's water retention improves as inflammatory signals decrease, allowing natural hyaluronic acid synthesis to increase. Joint fluid quality also improves as the inflammatory cascade that breaks down existing HA gets interrupted. This creates a positive feedback loop where supplementation supports your body's own HA production rather than replacing it.
Bioavailability challenges with high molecular weight HA have led to innovative delivery systems that preserve molecular size while improving absorption. Liposomal encapsulation protects large HA molecules during digestion, while specialized oral formulations use protective coatings to deliver intact high molecular weight compounds to target tissues. These advances make it possible to get anti-inflammatory benefits from oral supplementation, not just topical applications.
A meta-analysis of seven randomized controlled trials found that oral hyaluronic acid supplementation significantly improved skin hydration when molecular weight and dosing were optimized [4]. The studies that showed the strongest effects used high molecular weight formulations at doses between 120-240 mg daily, taken with meals to enhance absorption. Lower doses often failed to reach therapeutic thresholds, while higher doses didn't provide proportional benefits.
Individual Variation: The Hyaluronidase Factor
Your body's production of hyaluronidase, the enzyme that breaks down hyaluronic acid, varies dramatically between individuals and determines how well any HA supplement will work for you. Some people produce high levels of this enzyme, rapidly degrading supplemental hyaluronic acid before it can provide benefits. Others have lower hyaluronidase activity, allowing HA supplements to remain active for extended periods and provide more pronounced effects.
Genetic variations in hyaluronidase expression explain why identical supplement protocols produce different outcomes between people. High hyaluronidase producers often need higher doses or more frequent dosing to overcome rapid breakdown, while low producers may achieve better results with standard doses. This individual variation is one reason why clinical trials show wide confidence intervals and why personalized approaches to HA supplementation are becoming more important.
Age, hormonal status, and inflammatory conditions all influence hyaluronidase activity in your body. Estrogen decline during menopause increases hyaluronidase production, which is why postmenopausal women often need higher HA doses to achieve the same benefits as younger individuals. Chronic inflammatory conditions also upregulate hyaluronidase, creating a situation where the people who most need HA supplementation are also most likely to break it down quickly.
Environmental factors can temporarily increase hyaluronidase activity, reducing supplement effectiveness. UV radiation, air pollution, and psychological stress all boost enzyme production, explaining why HA supplementation may work better during certain seasons or life circumstances. Understanding these patterns helps optimize timing and dosing for maximum benefit. Some people find that splitting their daily dose between morning and evening provides more consistent effects than single large doses.
Dosing Strategies: Beyond the One-Size-Fits-All Approach
Your response to an HA supplement can vary because your body breaks HA down at different speeds. A key driver is hyaluronidase, the enzyme family that cuts HA into smaller fragments.
If you have higher hyaluronidase activity, you may break down supplemental HA faster. That can reduce how long intact HA stays available. It can also shift the mix toward smaller fragments, which may matter if you are trying to avoid pro-inflammatory signaling.
Several factors can influence hyaluronidase activity, including age, hormonal shifts, and baseline inflammation. That helps explain why two people can take the same product and get opposite results.
Practical takeaway: if you do not feel benefits after several weeks, you can trial a higher-MW product, split dosing, or a protected delivery form (like enteric-coated or liposomal) before assuming “HA doesn’t work for you.”
Synergistic Combinations: Enhancing HA Effectiveness
HA dosing works best when you match three things: your goal, your HA size (molecular weight), and your schedule.
For skin hydration support, studies that show benefits commonly use around 120–240 mg per day of oral HA [4]. Many people do well splitting the dose (for example, 60–120 mg twice daily) with meals.
For joint support, trial ranges in studies often fall around 80–200 mg per day, with changes taking longer than skin outcomes. Expect weeks, not days.
Be careful with “pulse dosing” claims. This article previously cited a trial where 400 mg every three days matched 120 mg daily for people with high enzyme activity [5]. Without clear confirmation in the provided study details, treat pulse dosing as experimental. If you try it, track your response carefully and keep the weekly total dose similar.
Topical vs. Oral: Delivery Method Impacts
The delivery method you choose for hyaluronic acid supplementation fundamentally alters its molecular weight profile and biological effects, making the topical versus oral decision crucial for achieving your specific goals. Topical HA formulations can preserve high molecular weight molecules that would be broken down during digestion, allowing for direct anti-inflammatory effects in skin tissue. However, penetration depth limits topical HA to superficial skin layers unless specialized delivery systems are used.
Oral HA supplementation faces the challenge of surviving digestive enzymes that preferentially break down larger molecules, often converting high molecular weight HA into smaller, potentially inflammatory fragments. This digestive breakdown explains why many oral HA supplements fail to provide the anti-inflammatory benefits seen in topical studies. Advanced oral formulations use enteric coatings or liposomal delivery to protect molecular integrity during digestion.
A systematic review of nine studies involving 278 participants found that specific topical HA formulations led to statistically significant improvements in skin hydration across multiple body regions [6]. The most effective formulations used cross-linked high molecular weight HA that resisted enzymatic breakdown while maintaining penetration capability. These results highlight the importance of formulation technology in determining supplement effectiveness.
The timing of effects differs significantly between delivery methods, with topical applications showing benefits within hours while oral supplementation requires days to weeks for noticeable changes. Topical HA immediately increases skin surface hydration and can reduce inflammatory markers in the epidermis within 2-4 hours of application. Oral HA must first be absorbed, distributed to target tissues, and accumulate to therapeutic levels before benefits become apparent, typically requiring 2-4 weeks of consistent use.
Combination approaches using both topical and oral HA can provide complementary benefits, with topical applications addressing immediate skin hydration needs while oral supplementation supports systemic tissue HA levels. This dual approach is particularly effective for comprehensive anti-aging protocols where both surface appearance and deeper tissue health are priorities.
Clinical Evidence: What the Latest Research Reveals
The strongest evidence for HA and skin hydration comes from topical and injection studies, not oral capsules. A meta-analysis of six studies found HA injection improved skin hydration (SMD = 1.34; 95% CI 0.14 to 2.54; p < 0.05) [7]. That supports HA’s biological ability to increase hydration.
For supplements you swallow, evidence is improving as studies better specify molecular weight and dose. A meta-analysis of seven randomized controlled trials found oral HA supplementation significantly improved skin hydration [4]. The size of the effect varies by study design, dose, and the HA form used.
Overall, HA appears well-tolerated in trials, with side effects usually mild when they happen (often stomach upset at higher doses). Longer-term data is still limited, but available studies do not suggest common serious harms.
Choosing the Right Formulation: A Practical Guide
To pick a hyaluronic acid supplement that matches your goal, start with one label question: does it state molecular weight (kDa)? If it does not, you cannot tell whether you are buying mostly high-MW chains, low-MW fragments, or a mix.
For calmer, anti-inflammatory signaling goals, look for high molecular weight HA (often listed as >1,000 kDa). For oral products, also look for a delivery approach meant to protect the molecule through digestion, such as enteric-coated or liposomal formats.
Quality control matters because HA can degrade over time and during processing. Prefer brands that share third-party testing or a certificate of analysis that includes purity and, ideally, molecular weight distribution.
If you choose a combination product (HA plus vitamin C, magnesium, or omega-3s), make sure the HA dose is still in the studied range (commonly 120–240 mg/day for skin hydration) and the molecular weight is disclosed.
Conclusions
Molecular weight is the hidden variable that often decides if an HA supplement helps you or irritates you. Evidence summarized in recent reviews links low molecular weight HA with higher IL-6 signaling in eligible studies, while high molecular weight HA is linked with higher IL-10 signaling. If your goal is skin hydration or joint comfort, a practical starting point is a high-MW HA product (>1,000 kDa) at 120–240 mg per day, ideally with a delivery form that helps protect the molecule. If you get no benefit, the next lever to adjust is not “more HA,” but a clearer molecular weight, better formulation, and a dosing schedule you can stick with.
Many cited studies measure inflammatory signals in cell, animal, or localized (topical/eye) settings, which may not translate directly to oral capsules. Several trials and reviews do not standardize or clearly report HA molecular weight, making head-to-head comparisons hard. Claims about exact timing of IL-6 changes after oral dosing and specific pulse-dosing equivalence are not well-established from the provided citations. Longer-term oral safety and effectiveness data beyond 12 months is still limited, especially for newer delivery systems such as liposomal or enteric-coated HA.
Track this in your stack
See how hyaluronic acid relates to your health goals and monitor changes in your biomarkers over time.