
Why Your LDL Target Should Be Personal, Not Universal
New research reveals individual factors that determine optimal cholesterol levels
You have probably been told that one LDL cholesterol target is right for everyone.
The reality is far more personal. Your ideal LDL goal depends on your age, genetics, and unique combination of risk factors. In this episode, you’ll learn why a universal number can miss the mark, how to find your true target, and what science-backed steps you can take to protect your heart and immune system for years to come.
- Plant sterols
- Compounds that lower LDL by blocking some cholesterol absorption in your gut.
- Red yeast rice extract
- A fermented rice supplement that can lower LDL by reducing liver cholesterol production.
- LDL Cholesterol (calc)
- LDL cholesterol, the "bad cholesterol" that deposits in artery walls. elevated LDL is the primary driver of atherosclerosis and heart disease.
- Personal LDL target
- An LDL goal set from your total risk, not a single universal cutoff.
- HMG-CoA reductase
- A liver enzyme that controls how much cholesterol your body makes.
- Apolipoprotein B
- Apolipoprotein B, the protein component of atherogenic particles. Desirable <90 mg/dL (risk-dependent).
- Berberine
- A plant compound that can lower LDL and may improve insulin sensitivity.
- HMG
- A molecule whose associated enzyme, HMG-CoA reductase, is targeted to lower cholesterol production.
- insulin
- A pancreatic hormone essential for regulating carbohydrate and fat metabolism in the body.
- LDL
- Low-density lipoprotein is a blood particle that transports cholesterol to cells and tissues.
You might remember the last time you sat across from your doctor. Maybe it was during your annual check-up, or after a friend’s health scare pushed you to finally schedule that blood test. The nurse wrote your LDL cholesterol on a printout, circled a number, and said, you want to stay under one hundred. That was it. No talk about your family history, your age, or what actually makes your heart tick. It is easy to walk away believing that everyone should chase the same magic number. But your body, your life, and your risks are not one-size-fits-all.
Imagine two people. One is in their early forties, runs regularly, and has no family history of heart disease. The other is in their seventies, with a history of high blood pressure and a parent who had a heart attack. Should these two people have the same LDL target? Recent research says no. The science now shows that the risks and benefits of lowering LDL cholesterol depend on who you are, not just what your number is. That is the difference between treating a lab value and truly protecting your future.
Focusing only on a universal LDL goal can lead to missed risks, wasted effort, or even unnecessary medication. You deserve a plan that matches your actual biology. To get there, you need to know what shapes your true heart risk, and how science lets you personalize your approach. That brings us to why your LDL target should reflect more than just a single number.
Your cholesterol is not just a number in a vacuum. It is a moving piece in the story of your body’s health—a story shaped by your age, genes, and the way your immune and metabolic systems work together. The reason your LDL goal should be personal is that the risk of heart disease and stroke changes dramatically as you age, and as your background risk factors stack up or shrink down.
Here is how it works. Cholesterol, especially the LDL type, is essential for your cells and hormones. But too much LDL can sneak into the walls of your arteries, where it triggers inflammation and plaque buildup over years. The more inflammation you have, the more likely these plaques are to rupture and cause a heart attack or stroke. But not everyone’s arteries respond the same way. If you are younger, with fewer risk factors, your arteries might be more resilient. If you are older, or if you have a family history of early heart disease, diabetes, or high blood pressure, your arteries are more vulnerable, and the same LDL level can do much more harm.
A landmark series of studies out of Copenhagen followed tens of thousands of adults across decades. These trials found that lowering LDL cholesterol helps everyone, but the absolute benefit is much bigger for people at higher risk—like those over sixty or with multiple risk factors. In other words, a small drop in LDL can prevent more heart attacks in someone at high risk than a big drop in someone at low risk. Your biology, not just your cholesterol, decides how much you stand to gain from targeting LDL more aggressively.
Genetics enter the picture too. Some people inherit versions of the PCSK9 gene or other variants that make their bodies naturally better or worse at clearing LDL from the blood. Others have a genetic tendency toward higher Lp(a), a form of cholesterol that raises risk regardless of your LDL. And for people with metabolic syndrome or chronic inflammation, the particles carrying cholesterol become smaller and denser, making them more dangerous.
This is why one-size-fits-all targets miss the mark. You need to know your personal risk story, so you can set a goal for LDL that actually protects your heart and immune system. Understanding your risk is the first step. Next, let’s look at the biomarkers that give you the full picture.
You may have heard the phrase, know your numbers. But when it comes to heart health, which numbers matter most? LDL cholesterol is just the start. To truly understand your risk, you need a set of biomarkers that reveal the full landscape—not just the LDL level, but the number and type of cholesterol particles, your genetic risk, and the presence of inflammation.
Let’s break down the key markers.
First, LDL cholesterol. For a healthy adult with few risk factors, an LDL below one hundred milligrams per deciliter is commonly recommended. But as you have heard, this is not the right target for everyone. If you have a family history of early heart disease, or if you are over sixty-five, studies show that lowering LDL to below seventy can deliver extra protection. The so what: your target should fit your risk, not just the average person.
Next, ApoB. This is a protein found on every atherogenic particle in your blood. Think of ApoB as the actual headcount of the particles that can cause plaque. Research shows that ApoB is often a better predictor of risk than LDL alone. If your ApoB is below eighty milligrams per deciliter, your risk is low. If it is above one hundred, you may need to get more aggressive, even if your LDL seems okay. The so what: ApoB tells you if your LDL number is truly safe for you.
Lp(a), or lipoprotein little a, is the next piece of the puzzle. This marker is almost entirely set by your genes and barely responds to diet or exercise. High Lp(a)—usually above fifty milligrams per deciliter—raises your risk by two to three times, even if everything else looks good. The so what: if you have high Lp(a), you may need to drive your LDL much lower to balance your risk.
Inflammation is the silent amplifier of heart risk. High-sensitivity C-reactive protein, or hsCRP, is your window into this process. A level below one milligram per liter is best. If your hsCRP is above two, your arteries are likely inflamed, and LDL particles are more likely to stick and cause damage. The so what: high inflammation means you are at higher risk, even if your LDL looks normal.
Other markers, like triglycerides and HDL cholesterol, also matter, but for most people, the big three are LDL, ApoB, and Lp(a), paired with hsCRP for inflammation. When you put these together, you get a risk profile that is as unique as your fingerprint.
So what does this mean for your next steps? It means you can set a target for LDL and related markers that truly matches your biology. That brings us to the supplements and protocols that science shows can help you reach those targets.
You have your numbers. Now, what can you do to move them in the right direction? Supplements can play a powerful role, but only when each one matches your personal driver of high LDL. The goal is to pick the right tool for your body’s unique cholesterol story.
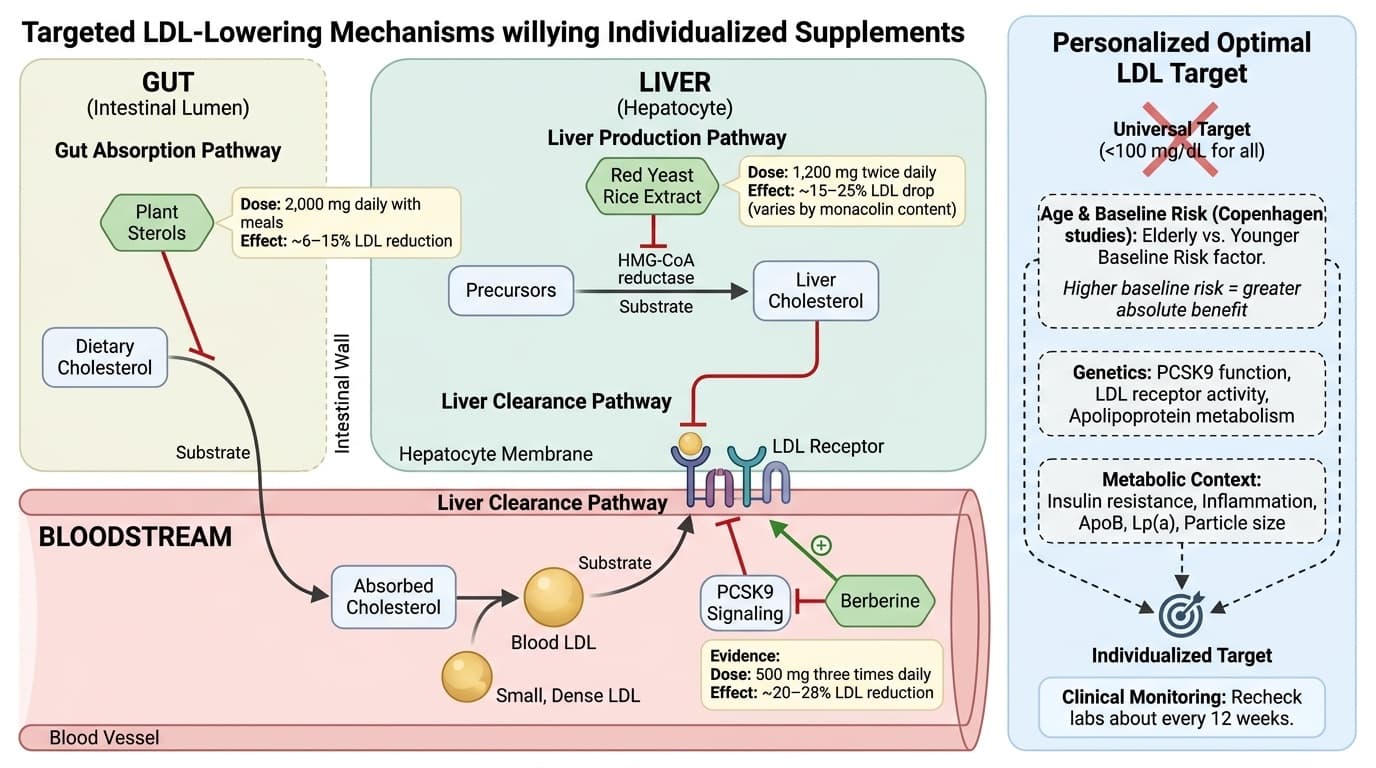
Let’s start with plant sterols. These are natural compounds found in vegetables and grains that block cholesterol absorption in your gut. Taking about two thousand milligrams daily with meals can lower LDL by six to fifteen percent, according to multiple clinical trials. The effect is strongest if your main issue is absorbing too much cholesterol from your diet. Mechanistically, plant sterols compete with cholesterol for absorption, so more leaves your body without entering your bloodstream. If you have high cholesterol but your diet is already healthy, plant sterols may help you get to your target.
Red yeast rice extract is another option, especially if your liver is making too much cholesterol. This supplement contains monacolins, natural compounds that block the HMG-CoA reductase enzyme—the same enzyme targeted by statin drugs. Studies using twelve hundred milligrams twice daily show drops in LDL of fifteen to twenty-five percent, though results depend on the specific product and the amount of monacolin present. Because red yeast rice works on liver production, it is a good fit if your labs suggest your body makes more cholesterol, regardless of what you eat. Mechanistically, it slows the biological assembly line that turns raw materials into cholesterol.
Berberine is a third option with multiple benefits. Berberine, at five hundred milligrams three times daily, can lower LDL by twenty to twenty-eight percent in some studies. It works by ramping up LDL receptor activity in your liver, pulling more LDL out of your blood, and also by modulating PCSK9, a protein that controls how much LDL your liver can clear. The bonus: berberine also helps lower blood sugar and improves insulin sensitivity, which is especially helpful if you have metabolic risk factors.
How do you know which to choose? If your absorption is high, plant sterols with soluble fiber work best. If your cholesterol is mostly made in the liver, red yeast rice is your go-to. If your metabolic risk is high, or you want to target both cholesterol and blood sugar, berberine makes sense. You can combine these, but always start one at a time and retest every twelve weeks to see how your numbers respond.
Supplements are not the whole story. They work best when paired with lifestyle changes, which can address root causes that no capsule can fix alone. Let’s look at those next.
Supplements can help, but your daily choices set the foundation for healthy LDL and a resilient immune system. The good news is that your heart and immune system respond quickly to changes in movement, food, and sleep.
Exercise is your first lever. Aim for at least one hundred fifty minutes each week of moderate aerobic exercise, like brisk walking, cycling, or swimming. This is not just about burning calories. Regular movement improves how your body processes fats and sugars, increases your HDL—the so-called good cholesterol—and makes your arteries more flexible. Mechanistically, exercise boosts the activity of enzymes that clear LDL from your blood, while also dialing down inflammation throughout your body. Even a brisk walk after dinner can make a difference.
Nutrition comes next. A heart-healthy plate is rich in vegetables, fruits, whole grains, nuts, seeds, and oily fish like salmon or mackerel. These foods provide fiber, antioxidants, and healthy fats that lower LDL by several pathways. Soluble fiber, found in oats, beans, and flaxseed, binds cholesterol in your gut and helps remove it before absorption. Omega-3 fatty acids from fish or algae lower triglycerides and reduce inflammation. Limiting saturated fat from red meats, butter, and processed foods puts the brakes on LDL production in your liver. Mechanistically, when you eat more plants and fewer processed foods, you lower the raw materials your body turns into cholesterol, and you help your immune system stay balanced and less inflamed.
Sleep is the often-overlooked third lever. Adults need seven to nine hours of sleep for optimal heart and immune function. Poor sleep raises stress hormones, increases inflammation, and makes it harder for your body to clear LDL. Mechanistically, deep sleep is when your body repairs vessel walls and resets immune cells. That is why sleep deprivation raises your heart attack risk, even if your cholesterol looks good on paper.
Lifestyle levers are powerful because they target the same mechanisms as medication and supplements, but with broader benefits. Each choice moves your numbers and your risk in the right direction. But what if things are starting to go wrong? That is where early warning signs come in.
Sometimes your body whispers before it shouts. The early signs of high LDL-related risk are usually subtle, but catching them early can save years of trouble down the road. Listening to these signs—and acting on them—can help you pivot before a problem becomes a crisis.
One key sign is family history. If a parent or sibling had a heart attack or stroke before age sixty, your risk is higher, even if you feel healthy. That puts you in the zone where more aggressive LDL lowering can pay off. Another sign is changes in your blood pressure, especially if you start trending higher over time. High blood pressure and high LDL work together to damage vessel walls, raising your risk faster than either one alone.
Metabolic changes can also tip you off. If your waist size is growing or you notice higher blood sugar, you may be entering a state of insulin resistance. This makes your LDL particles smaller and denser, which are more likely to cause plaque. Skin changes, like yellowish deposits around your eyes or tendons—called xanthomas—can be a rare but clear sign of very high cholesterol levels.
You should also watch for changes in your energy or exercise tolerance. If you feel more winded climbing stairs or need longer to recover after activity, these can reflect early changes in your heart and blood vessels, even before a doctor finds a problem. Inflammation-related symptoms, like frequent infections or slow healing, sometimes accompany high LDL and metabolic risk. That is because the same inflammation that drives heart disease can weaken your immune response.
If you see these signs, act early. Get a full set of labs, including LDL, ApoB, Lp(a), and hsCRP. Share your family history with your doctor. Ask about advanced testing if your story suggests higher risk. Early action is the difference between prevention and playing catch-up.
You have heard the advice for years—keep your cholesterol down, and you will be fine. But the truth is, what keeps you healthy is not a generic target. It is a strategy that fits your age, genes, and personal risk factors. Universal LDL goals make prevention easy to explain but easy to get wrong. Your risk is as personal as your fingerprints, and your plan should be too.
Modern science gives you the tools to measure your real risk. Biomarkers like ApoB and Lp(a) tell you if your LDL target should be lower than the standard advice. Inflammation markers like hsCRP show you if your immune system is quietly raising your risk, even when cholesterol looks okay. Supplements—like plant sterols, red yeast rice, and berberine—can help, but only when matched to your personal biology. Lifestyle levers, from daily movement to plant-based nutrition and good sleep, are powerful tools to shift your numbers and protect your arteries for decades to come.
The most important takeaway is this: you do not have to settle for a generic plan. Ask for the labs that give a complete picture. Set goals that reflect your story, not just the averages. Adjust your protocol based on how your numbers respond. And stay curious—because your health journey is ongoing. The earlier you act, the more options you have. Your future, your heart, and your immune system are worth the effort.
Ready to find your real LDL target and build your personalized plan? The science is here. The next move is yours.
Why Your LDL Target Should Be Personal, Not Universal
New research reveals individual factors that determine optimal cholesterol levels
Diagram glossary
- Berberine:
- A plant-derived compound used as a dietary supplement to improve metabolic and cholesterol profiles.
- HMG:
- A molecule whose associated enzyme, HMG-CoA reductase, is targeted to lower cholesterol production.
- insulin:
- A pancreatic hormone essential for regulating carbohydrate and fat metabolism in the body.
- LDL:
- Low-density lipoprotein is a blood particle that transports cholesterol to cells and tissues.
- monacolin:
- A naturally occurring statin-like compound found in red yeast rice that lowers cholesterol.
- PCSK9:
- An enzyme that binds to LDL receptors, targeted by drugs to lower blood cholesterol.
Conclusions
Your LDL goal should fit your risk, not a universal cutoff. Age, genetics, particle count (ApoB), Lp(a), and inflammation can all shift what “optimal” means for you. The most useful plan matches the tool to your main LDL driver—absorption, production, or metabolic risk—then tracks results and adjusts. With options like plant sterols, red yeast rice extract, and berberine, you can build a more precise LDL strategy than a one-number target.
Evidence for “personal LDL targets” is still evolving. Many findings come from observational research and post-hoc analyses, not trials that assign people to different LDL goals. Supplement studies also vary by product quality, dose, and study length, so LDL changes can differ from one brand and person to another. Finally, advanced markers like ApoB, Lp(a), and LDL particle tests are not always available, which can limit how personalized a plan can be.
Track this in your stack
See how ldl cholesterol relates to your health goals and monitor changes in your biomarkers over time.
Sources (2)
This article informs how supplementation moves 1 marker.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.