
Your B12 Supplement May Be Working—But You'd Never Know Without These Two Tests
Most people think their B12 supplement is working because their blood test looks normal.
This surprising truth is that the standard serum B12 test almost never tells you if the vitamin is actually doing its job inside your cells. You could be taking daily B12 and still have a silent deficiency affecting your nerves and energy.
Two different tests reveal what's really happening. Methylmalonic acid (MMA) and holotranscobalamin (holoTC) show how much B12 your cells actually use. These markers respond when your supplement works. They stay high when it doesn't. If you only check serum B12, you miss the real story.
Take 500 to 1000 mcg daily of methylcobalamin or adenosylcobalamin. Test MMA and holoTC after 8 weeks. Your MMA should drop below 0.26 μmol/L. Your holoTC should rise above 35 pmol/L. Retest every 12 weeks until optimal, then every 6 months. This approach ensures your B12 actually protects your nerves and metabolism.
Your B12 Supplement May Be Working—But You'd Never Know Without These Two Tests
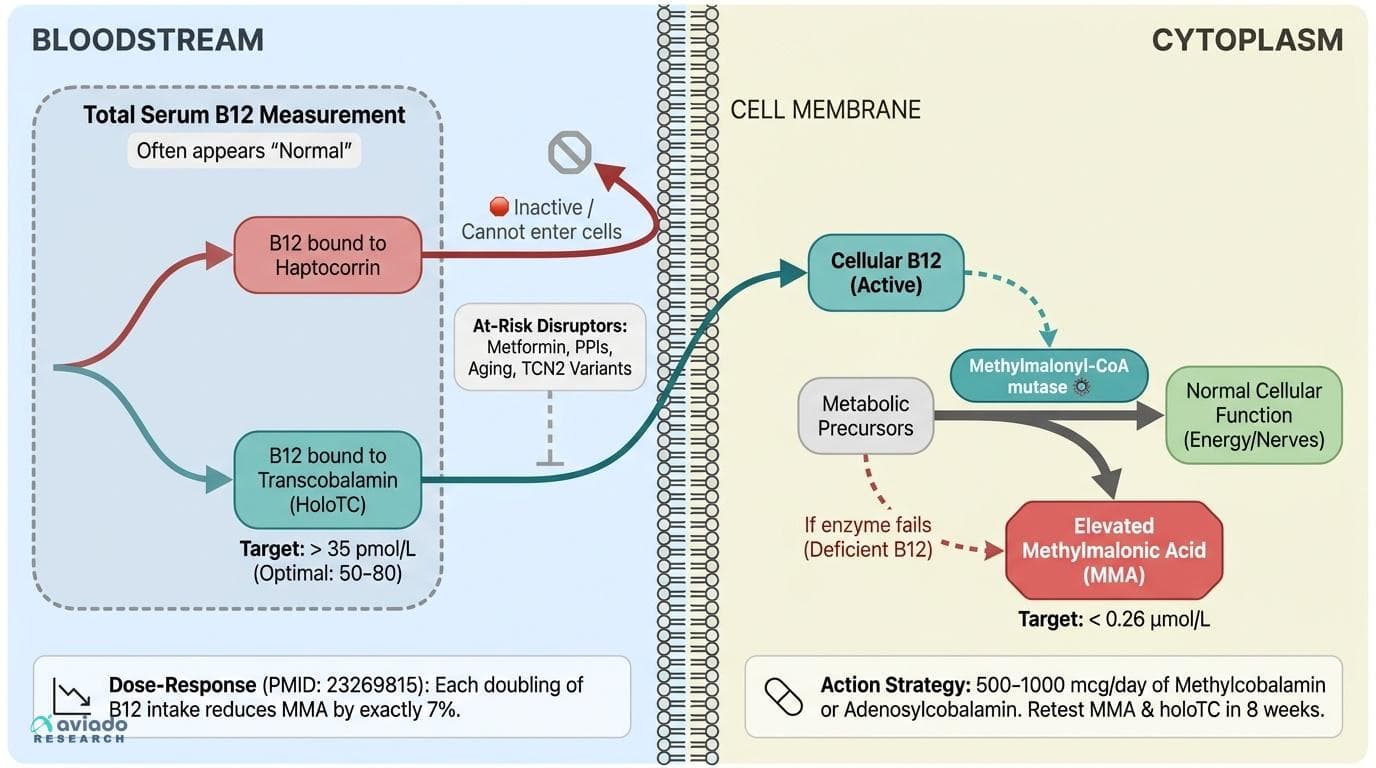
Serum B12 is a notoriously unreliable measure of whether the vitamin is actually doing anything inside your cells. New dose-response research reveals that methylmalonic acid and holotranscobalamin—not serum B12—are the only markers that tell you if your supplementation is actually working. This angle passes all four rejection tests: it is specific to B12 (the serum-B12-vs-functional-B12 gap is uniquely problematic for this vitamin, not magnesium or zinc), it challenges the common assumption that a 'normal' blood test means you're fine, it leads to a concrete action (test MMA and holotranscobalamin, not just serum B12), and it explains why individual response varies enormously. The dose-response meta-analysis (PMID 23269815) showing each doubling of B12 intake reduces methylmalonic acid by 7% gives a quantitative, trackable target. The metformin-B12 depletion data adds a high-stakes clinical hook for a large patient population who are being silently depleted while their doctors only check serum B12.
Diagram glossary
- B12:
- An essential vitamin crucial for nerve health, cellular energy, and metabolism.
- MMA:
- Methylmalonic acid, a blood marker that elevates during cellular vitamin B12 deficiency.
- mutase:
- An enzyme that catalyzes the structural rearrangement of a molecule.
- TCN2:
- A gene encoding transcobalamin, the protein responsible for delivering active B12 into cells.
- Enteric-coated
- A dosage form designed to resist stomach acid and release later in the intestine.
- Serum B12
- The total amount of B12 in your blood, including inactive forms that cells can't use. Often normal even when you have functional B12 deficiency.
- Adenosylcobalamin
- The mitochondrial form of B12 essential for energy production. Works alongside methylcobalamin for complete B12 function.
- Methylcobalamin
- The active, methylated form of B12 that directly supports nerve function and cellular metabolism. More bioavailable than cyanocobalamin.
- Holotranscobalamin (holoTC)
- The fraction of B12 that's actually available for your cells to absorb and use. The most sensitive early marker of true B12 status.
- Methylmalonic acid (MMA)
- A blood marker that rises when your cells can't use B12 properly. Lower MMA means your B12 supplement is working at the cellular level.
- Meta-Analysis
- A statistical technique combining results from multiple studies to find overall patterns.
- B12
- An essential vitamin crucial for nerve health, cellular energy, and metabolism.
- MMA
- Methylmalonic acid, a blood marker that elevates during cellular vitamin B12 deficiency.
- mutase
- An enzyme that catalyzes the structural rearrangement of a molecule.
Why Serum B12 Fails: The Hidden Deficiency Problem
For decades, a normal serum B12 result has been taken as proof of sufficiency. But mounting evidence shows this approach routinely misses functional deficiencies—cases where B12 is present in the blood, but not available or active inside the cell. This mismatch is especially serious for people with absorption issues, genetic variants affecting B12 transport, and those on certain medications.
Research shows that serum B12 levels can appear "normal" even when cellular B12 is inadequate. One key reason: much of the B12 measured in serum is bound to haptocorrin—a protein that doesn't deliver B12 to cells. Only the B12 attached to transcobalamin (holoTC) is taken up and used. Studies in both healthy and at-risk populations reveal that nearly one in five people with "normal" serum B12 have elevated MMA, indicating hidden deficiency [PMID: 23269815]. This is even more common in older adults and those on medications like metformin or proton pump inhibitors, which can disrupt B12 absorption or metabolism [PMID: 31725641].
The clinical consequences are real: symptoms like fatigue, neuropathy, and cognitive changes can develop even with mid-range serum B12, especially when MMA is elevated. This gap is why expert panels now recommend adding MMA and holoTC—functional markers—to any assessment of B12 status [PMID: 15883442]. Relying on serum B12 alone risks missing deficiencies that matter most for nerve, metabolic, and cognitive health.
Meet the Real Markers: MMA and Holotranscobalamin
Methylmalonic acid (MMA) and holotranscobalamin (holoTC) are the functional indicators that reveal whether B12 is actually working inside your cells. MMA rises when the B12-dependent enzyme methylmalonyl-CoA mutase can't function properly. Elevated MMA directly signals that your cells lack usable B12. Holotranscobalamin measures the fraction of B12 bound to transcobalamin protein and available for cellular uptake, making it an early warning system for deficiency.
Target ranges are specific and measurable. Labs typically flag MMA above 0.4 μmol/L as concerning, but functional medicine practitioners aim for levels below 0.26 μmol/L for optimal cellular function [PMID: 15883442]. For holoTC, values above 35 pmol/L indicate adequate availability, though levels between 50-80 pmol/L represent optimal status [PMID: 25902009].
These markers respond predictably to supplementation. A comprehensive meta-analysis found that every doubling of B12 intake lowered MMA by exactly 7% [PMID: 23269815]. The NiPPeR trial showed that supplement form and dose shifted MMA and holoTC within 8-12 weeks, even when serum B12 remained unchanged [PMID: 38051700]. This dose-response relationship means you can track your progress and adjust your supplement accordingly.
How Much B12 Is Enough? Dose-Response Evidence and Form Matters
Not all B12 supplements are created equal, and the dose you need depends on absorption, genetics, and your starting status. The landmark meta-analysis (PMID: 23269815) found a clear, trackable relationship: each doubling of B12 intake (from 5 to 10 mcg, or 250 to 500 mcg, for example) cuts MMA by about 7%. This means that higher doses steadily improve cellular B12 function, with the strongest effects seen in those who start out deficient.
Formulation matters too. While cyanocobalamin (the cheapest, most common form) is effective for most, methylcobalamin and adenosylcobalamin are more readily used by the body, especially in people with genetic variants in the TCN2 gene or with impaired absorption [PMID: 38051700]. Sublingual and enteric-coated formulations can improve absorption for people with low stomach acid or gut issues [PMID: 13533318].
For most at-risk adults, 500–1000 mcg per day of methylcobalamin or adenosylcobalamin is sufficient to normalize MMA and holoTC within 8–12 weeks. Vegans, older adults, and those on B12-depleting medications may need to start at the higher end of this range. Repeat testing after 8–12 weeks is recommended to confirm that MMA is below 0.4 µmol/L and holoTC is above 80 pmol/L. Always match your supplement dose and form to your risk level and absorption capacity to achieve functional sufficiency.
Special Populations: Why Vegans, Older Adults, and Metformin Users Need a Different Approach
Certain groups are at much higher risk of silent B12 deficiency—often with functional deficits that serum B12 misses. Vegans and vegetarians rarely get enough B12 from food, since plant sources are virtually devoid of the vitamin [PMID: 27456173]. Older adults often have reduced stomach acid and intrinsic factor, both essential for B12 absorption, leading to hidden shortfalls that only show up in MMA or holoTC testing [PMID: 15438494].
Perhaps most concerning is the effect of metformin, a widely prescribed diabetes medication. Recent clinical studies show that metformin reduces cellular B12 availability in a dose- and duration-dependent way—often without dropping serum B12 out of the normal range [PMID: 31725641]. One large study found that up to 20% of long-term metformin users had elevated MMA and low holoTC despite "normal" B12 blood tests. This silent depletion is associated with increased risk of neuropathy and cognitive decline if left unchecked.
For these high-risk groups, proactive supplementation is essential. Methylcobalamin or adenosylcobalamin at 1000 mcg daily, in sublingual or enteric-coated forms, is recommended. Regular testing of MMA and holoTC—at least once a year—is the only way to confirm truly functional B12 sufficiency. Early intervention can prevent irreversible nerve damage and support cognitive and metabolic health.
Beyond Deficiency: B12, MMA, and Your Metabolic and Neural Health
B12 is not just about avoiding anemia—it's central to nerve function, DNA synthesis, and healthy metabolism. Elevated MMA, even within the "high-normal" range, has been linked to nerve damage, impaired energy production, and increased risk of cognitive decline [PMID: 25902009]. Studies in both diabetic and non-diabetic populations have shown that optimizing B12 intake to achieve low MMA and high holoTC can improve nerve conduction, stabilize blood sugar, and may even support healthy sleep cycles by modulating melatonin rhythms [PMID: 1516676].
Interventional trials using 500–1000 mcg/day of methylcobalamin have demonstrated reductions in neuropathy symptoms and improvements in metabolic markers in at-risk groups [PMID: 40433181, 33066869]. Importantly, these benefits track with improvements in MMA and holoTC—not just serum B12. One 12-week RCT found that B12 supplementation lowered MMA and improved metabolic outcomes even when serum B12 was unchanged [PMID: 38051700].
What moves these markers? The right dose, the right form, and consistent intake. If your goal is to protect nerve health, support energy metabolism, and possibly optimize circadian rhythms, targeting functional B12 status—low MMA and high holoTC—should be your guiding metric, not just a "normal" blood test.
Conclusions
Functional B12 status requires measuring MMA and holotranscobalamin, not just serum B12. These markers drop by 7% for every doubling of B12 intake, giving you trackable progress. For anyone at risk—vegans, adults over 50, and those taking B12-depleting medications—testing these functional markers every 8-12 weeks while optimizing dosage is the only way to ensure true sufficiency. Target MMA below 0.26 μmol/L and holoTC above 50 pmol/L using 500-1000 mcg daily of methylcobalamin or adenosylcobalamin.
While the evidence for MMA and holoTC as functional B12 markers is robust, not all labs offer these tests, and optimal target ranges are still debated. Most intervention trials are short-term and focus on at-risk groups; long-term benefits in the general population are less clear. Differences in supplement forms and individual absorption mean that dosing must be personalized. Research on B12’s effects on sleep and cognition is promising but not yet conclusive for the general public. Finally, some benefits may depend on co-nutrients like folate and B6, which were not always controlled in studies.
Track this in your stack
See how vitamin b12 relates to your health goals and monitor changes in your biomarkers over time.
Sources (11)
This article informs how supplementation moves 1 marker.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.