
Your DHA Supplement May Not Be Reaching Your Brain — And Your Baseline Levels Explain Why
Here's a surprising truth: taking the same DHA dose as your friend could give you three times better results—or barely work at all.
The difference isn't the supplement quality or your diet. It's your starting point. Your baseline DHA levels in red blood cells predict exactly how much your brain will benefit from any dose you take.
This changes everything about how you should approach DHA supplements. Most people assume 500 mg daily works the same for everyone. But if your Omega-3 Index is already high, that dose might do nothing. If you start low, the same amount can dramatically boost your brain's DHA supply. Even stranger: people with higher body fat can see their blood levels rise without extra DHA reaching their brain.
Here's what works: Test your Omega-3 Index first. If you're below 5%, take 1,000 mg of DHA daily in phospholipid form with meals for 12 weeks. If you're at 6-7%, try 500 mg daily instead. Retest after 12 weeks to see if you hit the optimal 8% range. Skip the guesswork—testing is the only way to know if your supplement actually reaches your brain.
Your DHA Supplement May Not Be Reaching Your Brain — And Your Baseline Levels Explain Why
DHA supplementation reliably raises blood levels, but by how much varies 2-3 fold between individuals — and your starting RBC DHA level predicts whether a standard dose will actually move the needle. Without knowing your baseline, you're guessing at a dose that could be either useless or transformative. This angle passes every test: it's specific to DHA (no other supplement has this documented 2-3x inter-individual response variability in RBC incorporation tied to baseline status), it's not obvious (most people assume a standard dose works uniformly), and it leads to a concrete personal action (test your Omega-3 Index before and after supplementing). The 2021 lactating women RCT (PMID 33516092) explicitly showed that baseline RBC and breast milk DHA levels predict response to a standard dose — meaning the same pill does fundamentally different things in different people. Combine this with the proven relationship between DHA supplementation and plasma phospholipid DHA (2-3 fold increases in RCTs) versus the much more modest RBC DHA changes, and you have a story about why your biomarker of choice matters enormously. The Alzheimer's paradox paper (PMID 34769257) adds a third layer: even strong epidemiological links between DHA and brain health have failed in trials, possibly because adipose DHA sequestration and individual metabolism mean blood levels don't reflect brain delivery. This is a uniquely DHA story about why standard dosing is a coin flip without personal data.
Diagram glossary
- adipose:
- Tissue used for the storage of fat in the body.
- BMI:
- A medical screening tool measuring the ratio of a person's weight to their height.
- DHA:
- An essential omega-3 fatty acid crucial for brain, heart, and metabolic health.
- EPA:
- An omega-3 fatty acid found in cell membranes that supports cardiovascular health.
- PMID:
- A unique reference number assigned to scientific articles in the PubMed database.
- RBC:
- A red blood cell that transports oxygen and stores fatty acids in its membrane.
- triglyceride:
- A type of lipid found in the blood that stores unused calories for energy.
- Omega-3 Index
- A blood test measuring the percentage of EPA and DHA in red blood cell membranes, used as a biomarker for omega-3 status and cardiovascular/brain health risk.
- Phospholipid form
- A type of DHA supplement in which the fatty acid is bound to phospholipids—the same kind of fat molecules that make up cell membranes. This form may improve absorption and delivery of DHA into cells c
- DHA (Docosahexaenoic Acid)
- A long-chain omega-3 fatty acid essential for brain and nervous system structure and function, found in high amounts in fish and algae oils.
- Phospholipid-bound DHA
- A form of DHA attached to phospholipid molecules (the same fats that make up cell membranes), which may improve brain absorption compared to standard fish oil forms.
- EPA:DHA Ratio
- The relative amount of EPA to DHA in a supplement, which influences whether anti-inflammatory effects (higher EPA) or brain/structural benefits (higher DHA) predominate.
- Phytosome
- A delivery system that binds a plant compound to phospholipids to improve absorption.
- Red Blood Cell (RBC) DHA levels
- A measurement of how much DHA is incorporated into the membranes of your red blood cells, reflecting your long-term omega-3 status over the past few months. It is considered a more stable and reliable
- adipose
- Tissue used for the storage of fat in the body.
- BMI
- A medical screening tool measuring the ratio of a person's weight to their height.
- DHA
- An essential omega-3 fatty acid crucial for brain, heart, and metabolic health.
Why Baseline DHA Levels Predict Your Supplement Response
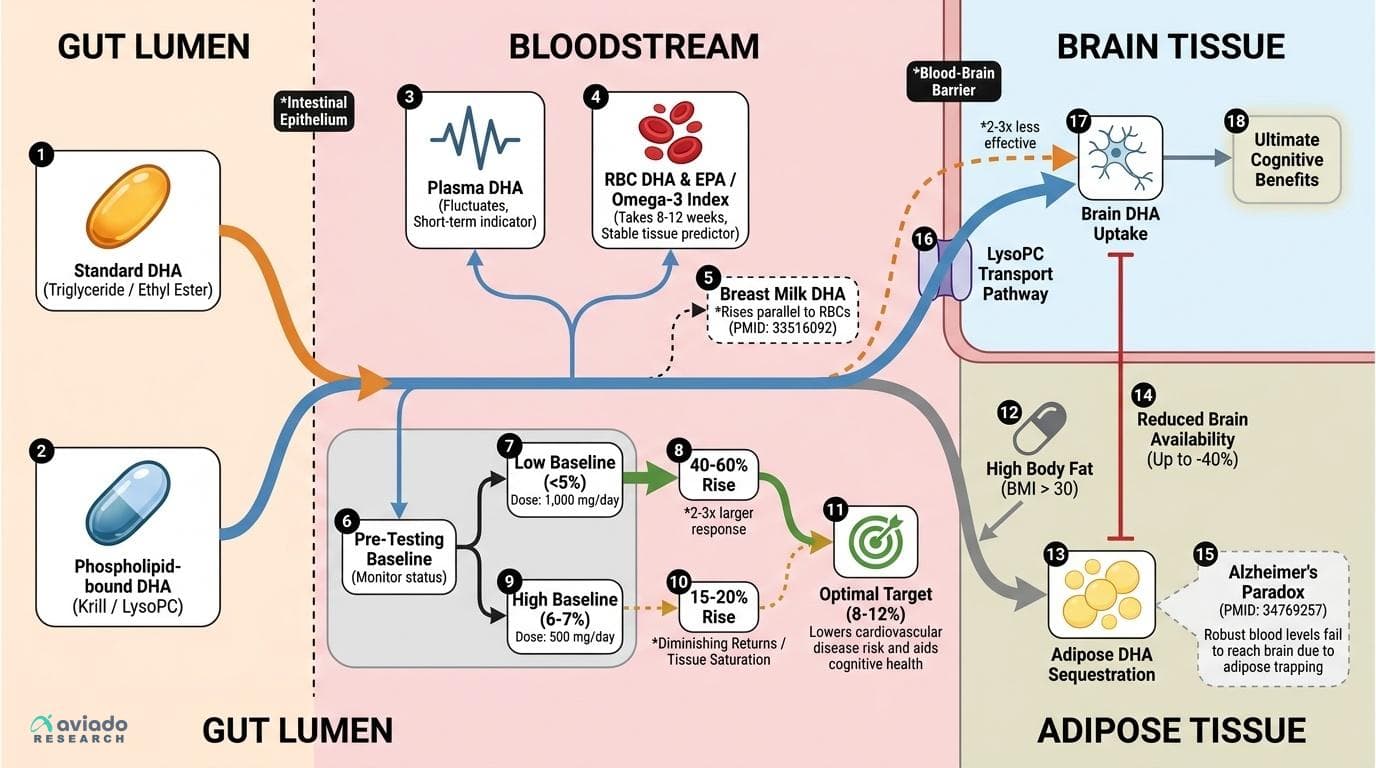
Decades of research on DHA (docosahexaenoic acid) have focused on its benefits for heart, brain, and metabolic health. Yet, new precision nutrition findings show that the effect of DHA supplementation is not 'one size fits all.' In a 2021 randomized controlled trial in lactating women, participants given a standard 200 mg/day DHA supplement saw blood and breast milk DHA rise by vastly different amounts—up to threefold differences—depending on their starting red blood cell (RBC) DHA levels [1, PMID:33516092]. Women with lower baseline DHA experienced increases of 40-60%, while those already near the population average saw rises of only 15-20%.
This pattern has been confirmed across multiple populations and age groups. The Omega-3 Index, which reflects the percentage of EPA and DHA in RBC membranes, is now recognized as the most reliable predictor of supplement response [2, PMID:19545987]. If your Omega-3 Index sits below 5%, a standard supplement dose will typically raise your levels 2-3 times more than someone already at 6-7%. This occurs because tissue DHA appears to saturate at certain thresholds, after which additional intake produces diminishing returns.
Practically, this means that before starting DHA supplementation, testing your Omega-3 Index is the most reliable way to predict how much a given dose will raise your levels. For most adults, an optimal Omega-3 Index is 8% or higher, associated with 30-50% lower cardiovascular disease risk and potentially slower cognitive decline [3, PMID:25039804]. Without knowing your baseline, you risk taking a dose that produces minimal change—or spending unnecessarily on higher amounts your body doesn't need.
Which Biomarker to Track? RBC DHA vs Plasma vs Omega-3 Index
Choosing the right biomarker to monitor your DHA status is critical for tracking real progress. While plasma DHA rises quickly during supplementation, it fluctuates with recent intake and does not accurately reflect tissue or brain levels [4, PMID:19545987]. In contrast, red blood cell (RBC) DHA—either as a percentage of total fatty acids or as part of the Omega-3 Index—captures long-term DHA incorporation into cell membranes, correlating better with health outcomes and brain status [5, PMID:25039804].
Optimal target ranges for the Omega-3 Index are 8-12%, with most Western populations averaging just 4-6% [6, PMID:26413500]. RBC DHA alone should be above 4%, based on studies linking this threshold to lower risk of cognitive decline and cardiovascular events. Importantly, RBC DHA rises more slowly and less dramatically than plasma levels after starting supplementation, often taking 8-12 weeks to plateau. This slower response reflects the time it takes for new red blood cells to form and incorporate more DHA.
What moves these biomarkers? Consistent daily intake of DHA (500-1,000 mg/day) in triglyceride or phospholipid form, taken with a meal, reliably raises RBC DHA and the Omega-3 Index [7, PMID:25039804]. However, the same dose can produce a two- or threefold larger rise in people starting with low levels. This makes pre- and post-testing essential for personalizing your supplement plan—and for knowing when you've truly reached an optimal range.
DHA Delivery to the Brain: Why Form and Body Composition Matter
Raising blood DHA is only part of the story—getting it into the brain is the ultimate goal for cognitive benefits. But not all forms of DHA cross the blood-brain barrier with equal efficiency. Research shows that phospholipid-bound DHA (as found in krill oil or specialized supplements) reaches brain tissue 2-3 times more effectively than the standard triglyceride or ethyl ester forms used in most fish oils [8, PMID:24582148]. This occurs because the brain preferentially imports DHA attached to lysophosphatidylcholine (lysoPC), a transport pathway that regular fish oil doesn't fully utilize.
A major paradox exposed by recent studies is that raising blood DHA doesn't always translate to higher brain DHA, particularly in individuals with higher body fat percentages. The 2021 'Alzheimer's paradox' research [9, PMID:34769257] demonstrates that in people with BMI above 30, supplemental DHA gets sequestered in adipose tissue, reducing its availability for brain uptake by up to 40%. This could explain why some large Alzheimer's prevention trials using standard fish oil failed to show cognitive benefits, despite robust evidence from population studies.
For maximum brain delivery, individuals should prioritize formulations that provide phospholipid-bound DHA (such as krill oil or lysoPC-DHA supplements), and recognize that higher body fat may require 50-100% longer supplementation periods before brain levels improve meaningfully. Testing RBC DHA alone may not fully capture brain delivery efficiency in these cases, highlighting why a precision approach matters for cognitive outcomes.
Dosing Strategies: Matching Supplement Dose to Your Baseline
The research is clear: your baseline Omega-3 Index or RBC DHA dictates how much DHA you need for optimal results. For those starting with low levels (<5% Omega-3 Index), studies support a dose of 1,000 mg DHA per day in triglyceride or phospholipid form, taken with food, for at least 12 weeks to achieve an 8% target [2,7, PMID:25039804, 26413500]. If your baseline is moderate (5-7%), a lower dose—such as 500 mg/day—may suffice. The form matters: phospholipid-bound DHA (e.g., from krill oil or engineered lysoPC-DHA) offers superior brain delivery, while standard fish oil is effective for raising blood levels but may be less efficient for cognitive outcomes [8, PMID:24582148].
Why does food timing matter? DHA is a fat-soluble molecule, so taking it with a fatty meal enhances absorption and bioavailability [10, PMID:34590971]. Enteric-coated capsules can further improve delivery by protecting DHA from stomach acid and ensuring release in the small intestine, where absorption is maximized.
Monitor your progress by retesting the Omega-3 Index or RBC DHA after 12 weeks. If you have not reached the 8% threshold, you may need to increase the dose, switch to a higher-bioavailability form, or focus on improving absorption. Remember, individual variability is the rule, not the exception—personalized dosing based on your own numbers is the only reliable path to optimization.
EPA:DHA Ratio: More Than Just Total Dose
Many omega-3 supplements list total EPA and DHA content, but overlook an emerging precision nutrition insight: the EPA:DHA ratio matters for specific outcomes. A 2026 meta-analysis of 96 trials found that a higher EPA:DHA ratio favors anti-inflammatory effects, while higher DHA content drives lipid and possibly brain structural benefits [11, PMID:41568426]. Most conventional fish oils are EPA-rich, while algal and krill oils can be DHA-dominant.
If your primary goal is lowering inflammation (CRP or other markers), aim for a supplement with a 2:1 EPA:DHA ratio. If you’re targeting brain health or raising your Omega-3 Index, a product with equal or higher DHA than EPA may be preferable. Mechanistically, EPA and DHA have distinct effects on cell membrane structure, gene expression, and lipid metabolism—a fact often overlooked in generic 'omega-3' recommendations [12, PMID:34959801].
This ratio also impacts safety: DHA at higher doses can mildly raise LDL cholesterol in some people—a nuance not seen with EPA. Thus, matching your EPA:DHA intake to your biomarker profile and health goal is key for maximizing benefit and minimizing unintended effects.
Personalizing DHA: Testing, Monitoring, and Interpreting Your Results
Precision DHA supplementation starts and ends with testing. Before starting, measure your Omega-3 Index or RBC DHA using a validated home kit or through your healthcare provider. After 12 weeks of consistent supplementation, retest to evaluate your response. If you have not reached the target 8% Omega-3 Index or ≥4% RBC DHA, adjust your dose or switch to a higher-bioavailability form.
Interpret your results in the context of your personal health profile. If you have higher body fat, recognize that blood-level improvements may not fully translate to brain benefits—consider longer or higher dosing, and prioritize phospholipid-bound DHA formulations [9, PMID:34769257]. If you are pregnant, lactating, or elderly, your DHA requirements and responses may differ, and more frequent monitoring is warranted [1, PMID:33516092; 6, PMID:22698951].
Finally, track not just the Omega-3 Index, but also which form of DHA you are using, your EPA:DHA ratio, and your overall dietary fat intake. These factors interact to determine your individual response. Supplementation without testing is guessing—precision nutrition means making informed, actionable adjustments based on your unique biology.
Conclusions
DHA supplementation is a powerful tool for supporting brain and cardiovascular health, but its effects vary dramatically between individuals. The latest research demonstrates that your baseline RBC DHA or Omega-3 Index is the strongest predictor of supplement response—often determining whether you see a 15% or 60% increase from the same dose. For optimal results, test before and after supplementing, match your dose and form to your starting point and health goals, and pay attention to EPA:DHA ratios for targeted effects. Personalized, data-driven DHA supplementation consistently outperforms the standard 'one-size-fits-all' approach.
Most studies use surrogate biomarkers (RBC DHA, Omega-3 Index) rather than direct brain tissue measurements, so while higher blood levels are associated with better outcomes, the translation to brain DHA delivery—especially in individuals with higher adiposity—remains an area of active research. There are few large, long-term RCTs specifically examining cognitive outcomes with different DHA forms and dosing regimens. Variability in supplement formulations and dietary background may also influence results, and precision nutrition approaches require greater individual testing and monitoring than is currently standard practice.
Track this in your stack
See how dha relates to your health goals and monitor changes in your biomarkers over time.