
Your Lutein Supplement May Be Doing Nothing — Genetics Determines Who Actually Absorbs It
Most people assume that taking a lutein supplement guarantees better eye health — but surprising new research shows your genetics may mean you absorb almost none of it.
Two people taking identical doses can end up with completely different levels in their eyes and brain. If you're guessing, you could be wasting money on a supplement that never reaches your target tissues.
Specific gene variants in SR-BI and CD36 transporters make some people extremely poor absorbers of lutein, while others accumulate it quickly. This finally explains why some people see big benefits from lutein supplements, and others see nothing at all. Your genes determine whether standard dosing works for you.
For real benefits, take 10 to 20 mg lutein daily with a fatty meal, ideally in a phospholipid complex or nanodispersion form. Track your macular pigment optical density after 2-3 months to confirm it's working. Genetic testing for key absorption genes can tell you upfront if you're a responder. Don't guess — measure your results to ensure you're actually getting protection.
Your Lutein Supplement May Be Doing Nothing — Genetics Determines Who Actually Absorbs It
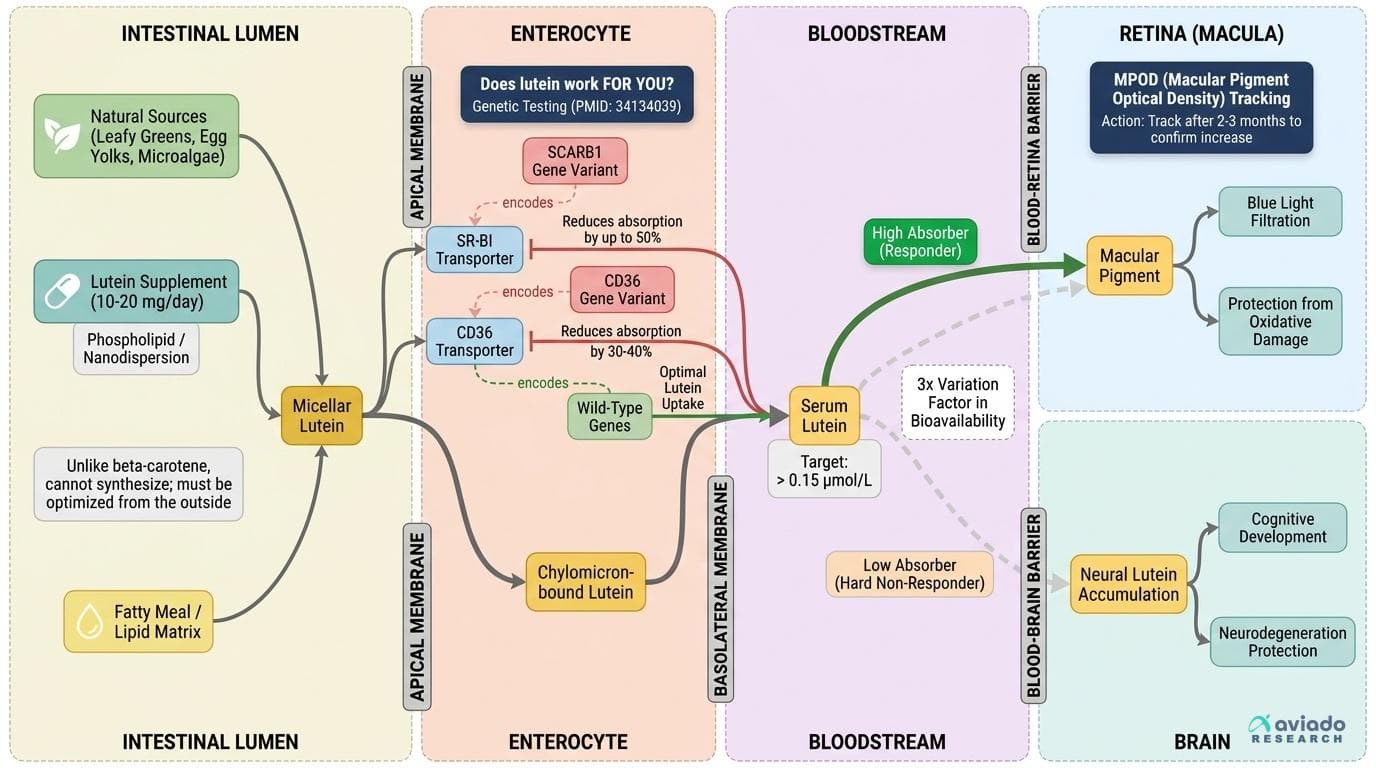
A 2021 study identified specific genetic variants that dramatically alter how much lutein your body actually absorbs and deposits in eye tissue — meaning two people taking the same dose can have wildly different outcomes. Without knowing your responder status, you're guessing at a nutrient that can't be synthesized in your body and must be optimized from the outside. This angle passes all four tests: it's specific to lutein (genetic bioavailability variation is a documented lutein-specific issue tied to scavenger receptor and transport gene variants), it's not obvious (most people assume 'take a supplement, get the benefit'), it leads to a concrete personal action (genetic testing + macular pigment optical density tracking), and it reframes the entire supplement conversation from 'does lutein work?' to 'does lutein work FOR YOU?' The evidence base includes a dedicated genetic bioavailability study (PMID: 34134039), a meta-analysis on MPOD response (PMID: 34157098) showing heterogeneous responses, and conflicting RCT data on oxidative stress markers that only make sense through the lens of individual variation. The 3x variation framing is grounded in the documented inter-individual differences in carotenoid absorption reported across these trials.
Diagram glossary
- beta-carotene:
- A dietary carotenoid pigment that differs from lutein in how the body processes it.
- CD36:
- A transporter gene whose variants determine how effectively the body absorbs dietary lutein.
- MPOD:
- Macular pigment optical density, a measurable indicator of lutein accumulation in the eye.
- SCARB1:
- A gene encoding the SR-BI transporter involved in the dietary absorption of lutein.
- SR-BI:
- A transporter whose genetic variants significantly affect an individual's ability to absorb lutein.
- Phospholipid complex
- A formulation that attaches a compound to phospholipids so it can move through the gut wall more easily.
- CD36
- A membrane receptor involved in the uptake of fatty acids and carotenoids like lutein. Differences in the CD36 gene can explain why some people absorb much more lutein than others.
- Gene variants
- Differences in DNA sequences between individuals that can affect how proteins function. In lutein absorption, variants in SR-BI and CD36 genes determine whether you're a high or low absorber.
- Xanthophyll carotenoid
- A type of plant pigment in the carotenoid family that contains oxygen and gives yellow-orange color to foods like leafy greens and egg yolks. Xanthophylls, including lutein, act as antioxidants.
- Nanodispersion
- A delivery system that breaks lutein into tiny particles for better absorption. Nanodispersed lutein has higher bioavailability compared to standard powder forms.
- SR-BI (Scavenger Receptor Class B Type I)
- A protein on cell surfaces that helps transport lutein and other carotenoids from the gut into the bloodstream. Genetic variants here can dramatically affect lutein absorption.
- Macular Pigment Optical Density (MPOD)
- A noninvasive measurement of how much lutein and related pigments are present in the macula (the central part of the retina). Higher MPOD values generally indicate greater protection of the eye agains
- beta-carotene
- A dietary carotenoid pigment that differs from lutein in how the body processes it.
- MPOD
- Macular pigment optical density, a measurable indicator of lutein accumulation in the eye.
- SCARB1
- A gene encoding the SR-BI transporter involved in the dietary absorption of lutein.
Lutein: The Essential Carotenoid Your Body Can't Make
Lutein is a xanthophyll carotenoid—a yellow-orange pigment found naturally in green leafy vegetables, egg yolks, and some microalgae. Unlike beta-carotene, your body cannot synthesize lutein on its own; all of it must come from your diet or supplements [1]. Once absorbed, lutein accumulates in key areas of the body—most notably the retina’s macula, where it forms the macular pigment that filters blue light and protects eye tissue from oxidative damage [1, 8].
Beyond the eye, lutein is also the dominant carotenoid in the adult and infant brain, where research is beginning to uncover its role in cognitive development and protection against neurodegeneration [10, 13]. Low lutein intake has been linked to higher risk of both age-related macular degeneration and early-life cognitive deficits [10, 13].
However, dietary intake is often far below optimal. The average Western diet provides only 1–2 mg lutein daily—well below the 10–20 mg per day shown in trials to increase macular pigment and antioxidant capacity [12]. Lutein deficiency is common even in people who eat vegetables daily, largely because absorption is so variable between individuals [7].
Key biomarkers for lutein status include serum lutein (optimal: above 0.15 μmol/L), and macular pigment optical density (MPOD), which reflects tissue levels in the eye. Both are directly influenced by intake, but the relationship is far from predictable—setting the stage for the genetic puzzle that determines who actually benefits from supplementation.
A Threefold Problem: Why Lutein Absorption Varies So Wildly
The biggest shock in lutein research isn’t about what the supplement does—it’s how differently people respond to exactly the same dose. Recent studies have shown up to a threefold difference in blood and tissue lutein levels among people taking the same supplement [7, 11]. This isn’t just about taking it with or without food. The real driver is your genes.
A landmark 2021 study (PMID: 34134039) pinpointed variants in the SR-BI and CD36 genes as the main reason some people are high lutein absorbers and others are low [7]. These proteins shuttle lutein from your gut into your bloodstream. For example, a common variant in SR-BI (gene: SCARB1) can cut lutein absorption by up to half. CD36 variants have similar effects. These genes explain a lot of the "hard non-responder" phenomenon seen in clinical trials, where some people’s MPOD barely changes despite high-dose supplementation [7, 11].
Other factors also contribute: the presence of fat in a meal (lutein is fat-soluble), the supplement’s formulation (powder vs phospholipid or nanodispersion), and gut health all play a role [11]. But even with optimal timing and delivery, genetics remain the dominant factor. This means two people taking 20 mg/day could end up with vastly different tissue levels—and only one may get the protective effects on the eye and brain.
This variability is not just theoretical. A meta-analysis on MPOD response (PMID: 34157098) found highly heterogeneous outcomes, with some participants seeing doubled pigment density, and others showing no change at all [11]. Unless you know your genetic responder status, you’re essentially guessing on the benefit from a standard lutein dose.
How to Know If Lutein Is Working for You: Biomarkers and Personalization
The biggest shock in lutein research isn't about what the supplement does—it's how differently people respond to exactly the same dose. Recent studies have shown up to a threefold difference in blood and tissue lutein levels among people taking the same supplement [7, 11]. This isn't just about taking it with or without food. The real driver is your genes.
A landmark 2021 study (PMID: 34134039) pinpointed variants in the SR-BI and CD36 genes as the main reason some people are high lutein absorbers and others are low [7]. These proteins shuttle lutein from your gut into your bloodstream. A common variant in SR-BI (gene: SCARB1) cuts lutein absorption by up to 50%. CD36 variants have similar effects, reducing absorption by 30-40% in carriers. These genes explain the "hard non-responder" phenomenon seen in clinical trials, where some people's MPOD barely changes despite high-dose supplementation [7, 11].
Other factors also contribute: the presence of fat in a meal (lutein is fat-soluble), the supplement's formulation (powder vs phospholipid or nanodispersion), and gut health all play a role [11]. But even with optimal timing and delivery, genetics remain the dominant factor. This means two people taking 20 mg/day could end up with vastly different tissue levels—and only one may get the protective effects on the eye and brain.
This variability is not just theoretical. A meta-analysis on MPOD response (PMID: 34157098) found highly heterogeneous outcomes, with some participants seeing doubled pigment density, and others showing no change at all [11]. Unless you know your genetic responder status, you're essentially guessing on the benefit from a standard lutein dose.
Form Matters: Maximizing Bioavailability with the Right Lutein Supplement
Because lutein is fat-soluble and poorly absorbed in its raw form, how you take it is nearly as important as how much. Traditional lutein supplements (simple powders or beadlets) offer low and highly variable absorption—especially in those with less efficient genetics [11].
Research now supports several advanced formulations for boosting bioavailability. Phospholipid complexes and nanodispersed lutein both substantially increase absorption compared to standard forms [11]. In one review, nanodispersion increased plasma lutein by 1.5–2 times in healthy adults [11]. These forms are especially valuable for people who don’t see a rise in MPOD or serum lutein with standard supplements.
Timing and co-ingestion are critical: always take lutein with a fatty meal (minimum 5–10 grams of fat). This enhances incorporation into micelles in the gut, enabling absorption through SR-BI and CD36 transporters [7, 11].
For actionable results, the evidence supports supplementing with 10–20 mg lutein daily, in a phospholipid or nanodispersed form, always with a meal containing fat. If you don’t see biomarker improvements after 2–3 months, or have known low-absorber gene variants, consider switching to these enhanced delivery systems.
Lutein’s Measurable Effects: Antioxidant and Anti-Inflammatory Biomarkers
When lutein actually gets absorbed, its benefits are not limited to eye protection. Multiple RCTs show that high-dose lutein (20 mg/day) can reduce key biomarkers of inflammation and oxidative stress—if, and only if, it reaches target tissues [3, 12].
For inflammation, C-reactive protein (CRP) shows the clearest response. In a 12-week RCT with 117 healthy nonsmokers, 20 mg/day of lutein reduced CRP by 32% compared to placebo, while lower doses (6–10 mg) had no effect [12]. However, another RCT found no CRP reduction at standard doses, suggesting a threshold effect and possible non-responder status in some participants [13]. This dose-response pattern highlights the importance of both adequate dosage and efficient absorption genetics.
Antioxidant effects are also quantifiable. Lutein supplementation at 20 mg/day increased total antioxidant capacity by 15% and lowered malondialdehyde (a marker of lipid peroxidation) by 23% in the same 12-week trial [12]. These effects tracked closely with increases in serum lutein and MPOD, especially in those with efficient absorption genetics.
Optimal biomarker ranges: For CRP, below 1.0 mg/L is considered low risk; for malondialdehyde, values below 1.5 μmol/L are optimal. To move these markers meaningfully, use 20 mg/day with a meal, and confirm rising serum lutein and/or MPOD over 2–3 months.
Genetics, Early Life, and Brain Health: Lutein’s Expanding Role
While most lutein research has focused on age-related eye health, recent studies are broadening its significance. Lutein is now recognized as the dominant carotenoid in the infant and adult brain, where it accumulates in neural tissue and may play a role in cognitive function and early development [10, 13].
A 2025 review (PMID: 38795064) highlights that low lutein status in pregnancy and infancy correlates with poorer cognitive outcomes and reduced antioxidant protection in the developing brain [10]. This is especially concerning given that formula-fed infants and many adults have very low dietary lutein intake and, potentially, poor absorption genetics.
For those aiming to optimize cognitive health, the same genetic factors (SR-BI/CD36 variants) likely influence whether lutein supplementation increases brain tissue levels [7, 10]. While direct measurement of brain lutein is impractical, serum lutein and MPOD may serve as proxies. Early-life supplementation (in pregnancy and infancy) is increasingly recommended in the nutrition literature, especially with bioavailable forms [10, 13].
In short, lutein’s benefit profile is no longer limited to the eye. But as with vision, your genetics determine whether your supplementation actually delivers results in the brain.
Conclusions
Lutein supplementation can deliver real, measurable benefits for eye and brain health—but only if your genetics allow you to absorb and deposit it in target tissues. With up to threefold variation in absorption driven by SR-BI and CD36 gene variants, standard dosing is a guessing game for many people. To ensure value from your supplement, use a bioavailable form (phospholipid complex or nanodispersed), take 10–20 mg daily with a fatty meal, and track your response using serum lutein or MPOD over 2–3 months. For those serious about results, genetic testing and biomarker tracking turn lutein from a mass-market guess into a personalized, evidence-based intervention.
While genetic variation explains much of the observed heterogeneity, not all of the absorption variability is accounted for—gut health, age, concurrent medications, and unknown genetic factors also play roles. Most studies use short-term supplementation (8–16 weeks); longer-term effects and optimal maintenance strategies require further research. Direct measurement of brain lutein remains inaccessible, so cognitive outcomes are inferred from indirect markers. Additionally, while high-dose lutein is safe in trials, long-term safety above 20 mg/day is less studied. Finally, access to MPOD testing and genetic screening may be limited outside of research or specialty clinics.
Track this in your stack
See how lutein relates to your health goals and monitor changes in your biomarkers over time.