
Your PLP Level Is a Hidden Report Card on Inflammation, Cancer Risk, and Metabolic Health — Most People Have Never Tested It
Here's something surprising: your PLP level might be the most telling blood marker you've never heard of.
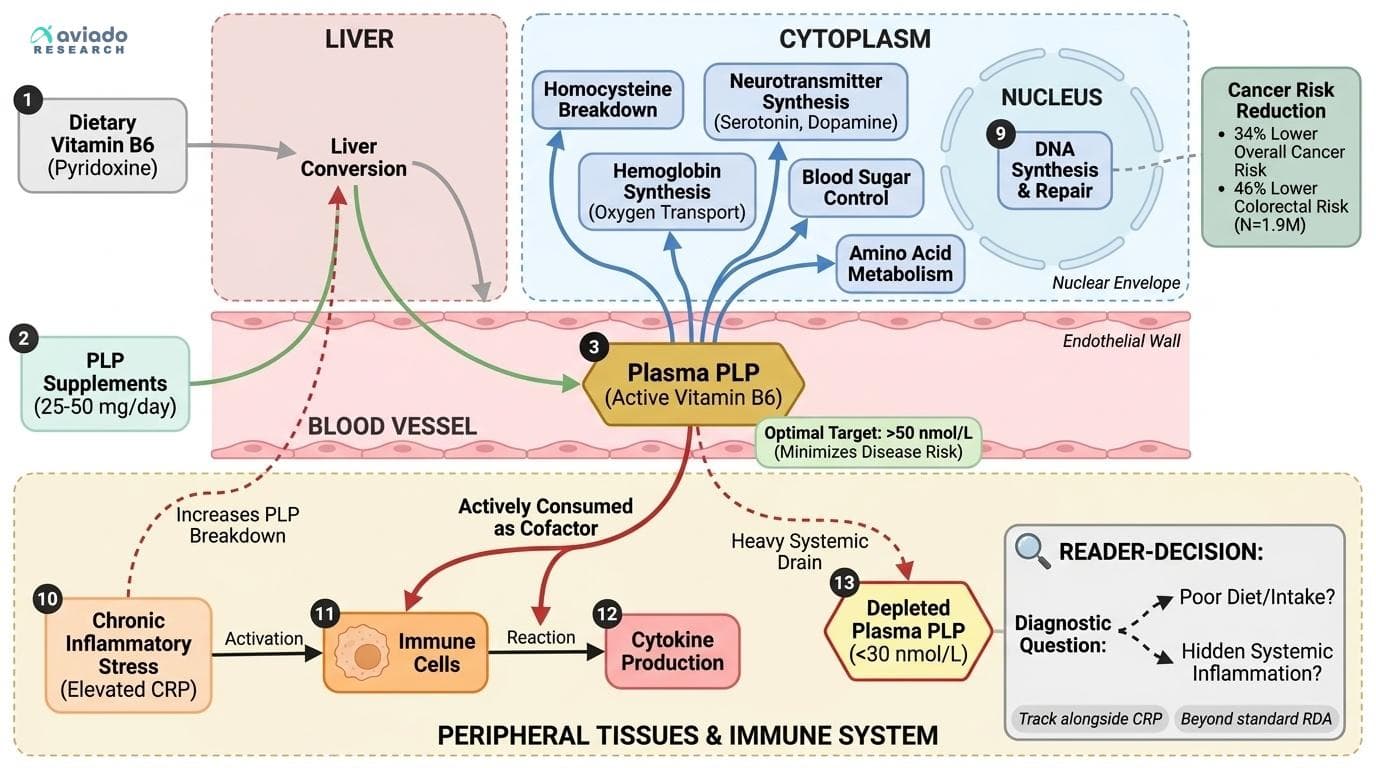
Most people assume low vitamin B6 means they need to eat more B6-rich foods. But new research reveals that inflammation itself burns through PLP (the active form of B6) at a rapid rate. So low PLP often signals hidden inflammation, not poor diet.
This matters because people with higher PLP levels have dramatically lower cancer risk. A study of nearly 2 million people found those with the highest PLP had 34% lower cancer risk overall and 46% lower colorectal cancer risk. Plus, PLP tracks your body's inflammation load better than standard tests. When inflammation spikes, PLP drops fast.
Here's what to do: Test your plasma PLP and aim for levels above 50 nmol/L. If you're low, take 25-50 mg daily of pyridoxal-5'-phosphate (not regular B6). Take it with food for better absorption. If your PLP stays low despite supplements, dig deeper into inflammation sources like gut problems or metabolic issues.
Your PLP Level Is a Hidden Report Card on Inflammation, Cancer Risk, and Metabolic Health — Most People Have Never Tested It
Pyridoxal-5'-phosphate (PLP), the active form of vitamin B6, is consumed by inflammation itself — meaning low PLP may not signal poor diet but rather a body under chronic inflammatory stress. A meta-analysis of 1.9 million people found high PLP associated with 34% lower cancer risk, yet almost no one tracks this biomarker. This angle passes all four tests: (1) UNIQUENESS — PLP as an inflammation-consumption biomarker is specific to B6 biology, not generic; (2) NOVELTY — the idea that low PLP may be a symptom of inflammation rather than a cause inverts the standard 'just take more B6' advice; (3) ACTIONABILITY — it directs readers to a specific, measurable, underutilized blood test; (4) READER-DECISION — it forces a concrete question: 'Is my low PLP due to poor intake or high inflammation?' which changes the intervention entirely. It also avoids the obvious 'high doses are bad' framing and instead reframes PLP as a diagnostic window into systemic health. The cancer-risk association (OR 0.54 for colorectal; RR 0.66 across 1.9M people) gives it dramatic stakes, while the inflammation-consumption mechanism explains why simply supplementing without tracking may miss the point.
Diagram glossary
- B6:
- An essential water-soluble vitamin involved in metabolism, neurotransmitter synthesis, and red blood cell production.
- cofactor:
- A non-protein chemical compound required for an enzyme's biological activity and metabolic reactions.
- CRP:
- A protein produced by the liver that serves as a biomarker for systemic inflammation.
- disease:
- An abnormal condition that negatively affects the structure or function of an organism.
- DNA:
- The molecule carrying genetic instructions for the development and functioning of all known organisms.
- dopamine:
- A neurotransmitter in the brain that regulates movement, reward, mood, and cognitive functions.
- homocysteine:
- An amino acid whose elevated blood levels are linked to cardiovascular and cognitive risks.
- oxygen:
- A chemical element essential for cellular respiration and carried by hemoglobin in the blood.
- PLP:
- Pyridoxal-5'-phosphate is the active coenzyme form of vitamin B6 essential for human metabolism.
- pyridoxine:
- A common supplement form of vitamin B6 that requires liver conversion to become active.
- RDA:
- The estimated amount of a nutrient considered adequate to meet daily dietary needs.
- TMAO (trimethylamine N-oxide)
- A gut-derived compound linked to cardiovascular risk; B6 may help lower it.
- Pyridoxamine
- Another form of vitamin B6 that shows particular promise for blood sugar control and diabetic complications.
- Inflammation-consumption hypothesis
- The idea that inflammation actively uses up and lowers PLP levels, so low PLP might reflect ongoing inflammation rather than just low intake.
- C-Reactive Protein (cardiac)
- High-sensitivity C-reactive protein, a liver-produced acute-phase reactant. Independent predictor of heart attack and stroke.
- Pyridoxal-5'-phosphate (PLP)
- The active, coenzyme form of vitamin B6 in the body. PLP is what actually does the biochemical work and is the best blood marker for B6 status.
- Homocysteine
- Homocysteine, an amino acid metabolite influenced by B vitamins. elevated levels damage blood vessels and increase cardiovascular and dementia risk.
- Pyridoxine
- The common supplemental form of vitamin B6, but less effective than PLP because it relies on liver conversion.
- B6
- An essential water-soluble vitamin involved in metabolism, neurotransmitter synthesis, and red blood cell production.
- cofactor
- A non-protein chemical compound required for an enzyme's biological activity and metabolic reactions.
- CRP
- A protein produced by the liver that serves as a biomarker for systemic inflammation.
PLP: The Active Form of Vitamin B6 and Why It Matters
Vitamin B6 is an umbrella term for six related compounds, but only one — pyridoxal-5'-phosphate (PLP) — actually powers the chemical reactions at the heart of human metabolism. PLP acts as a coenzyme for over 150 enzymes, orchestrating everything from amino acid metabolism and neurotransmitter synthesis to blood sugar control and immune cell function [1,4]. Unlike the more common supplement form, pyridoxine, PLP doesn't require conversion in the liver, making it the most direct and reliable way to impact B6 status in the body.
PLP's centrality means that even small drops in its level can ripple through dozens of metabolic processes. For instance, PLP is required for making serotonin and dopamine, so deficiency can affect mood and cognition. It's also needed for the breakdown of homocysteine — a marker linked to cardiovascular and cognitive risk — and for the synthesis of hemoglobin, which carries oxygen in red blood cells [1,8].
What's less appreciated is that PLP isn't just a passive marker of dietary intake. New evidence shows PLP is actively consumed by inflammatory processes. Inflammation triggers immune cells to use up PLP to make cytokines and defend the body, effectively draining the blood supply [6]. This means low PLP can signal a body under metabolic assault, even if you're getting enough B6 from food or supplements.
For practical tracking, plasma PLP is the most reliable biomarker. Optimal levels are generally considered 30–110 nmol/L, but many experts now recommend aiming for at least 50 nmol/L to minimize disease risk, particularly for cancer and cardiovascular disease [6,7]. Dietary intake alone can leave many people below this mark, especially if inflammation is present.
Inflammation-Consumption: Why Low PLP Means More Than Just Low B6 Intake
For decades, clinicians assumed that low PLP in the blood simply meant you weren’t getting enough vitamin B6 in your diet. But recent studies have upended this view, showing that inflammation itself consumes PLP, lowering your blood level regardless of how much B6 you take in [6,12].
This is known as the “inflammation-consumption hypothesis.” When your immune system is activated — by infection, chronic disease, obesity, or even intense exercise — immune cells draw on PLP as a cofactor to ramp up the production of cytokines and other signaling molecules. At the same time, inflammation also increases the breakdown of PLP in the liver, further depleting blood levels [6].
The clinical implication is profound: a low PLP result may not mean you need more B6, but rather that your body is battling a hidden inflammatory state. Large studies have found that PLP is consistently lower in people with high C-reactive protein (CRP), a classic inflammation marker, even when their B6 intake is sufficient [6,12]. This effect is seen in rheumatoid arthritis, diabetes, and even in people with metabolic syndrome.
What can you do? First, measure your plasma PLP — not just total B6 or pyridoxine intake. If your PLP is below 30 nmol/L, check for signs of inflammation or metabolic stress (elevated CRP, poor gut health, obesity). If you supplement and PLP remains low, focus on anti-inflammatory strategies (diet, exercise, gut support) alongside B6, rather than just increasing the dose. This approach is more targeted and evidence-based than the old “just take more B6 and forget it” advice [6,12].
PLP and Cancer Risk: Evidence From 1.9 Million People
One of the most striking findings of the past decade is the link between PLP status and cancer risk, especially colorectal cancer. A comprehensive meta-analysis pooling data from nearly 1.9 million people found that those with the highest PLP levels had a roughly 34% lower risk of all cancers and a 46% lower risk of colorectal cancer specifically [12,11].
How could vitamin B6, or more precisely, PLP, wield such broad anti-cancer effects? Mechanistically, PLP is critical for DNA synthesis and repair, the breakdown of potentially carcinogenic compounds, and the control of cell division. PLP also helps keep inflammation in check, and chronic inflammation is a major driver of cancer initiation and progression [12,15].
Importantly, it’s not just low intake but low blood PLP that predicts higher cancer risk. Several large population studies adjusted for dietary B6 and still found that low PLP flagged higher risk — supporting the idea that inflammation-driven PLP depletion is part of the cancer risk story [11,12].
What does this mean for intervention? The protective association was strongest in people with PLP above 50 nmol/L, but benefits appear up to about 110 nmol/L. Supplementation with 25–50 mg/day of pyridoxal-5'-phosphate is safe and effective for raising PLP, especially in those at risk for deficiency or with chronic inflammation [7,12]. If you’re aiming for long-term cancer risk reduction, tracking and optimizing PLP is a data-driven strategy that goes well beyond the outdated “get your RDA” advice.
Beyond Cancer: PLP, Metabolic Health, and the Exercise Mimetic Effect
PLP’s influence extends far beyond cancer. Recent research reveals that marginal B6 deficiency — common in aging, obesity, and metabolic syndrome — is linked to increased risk of diabetes, cardiovascular disease, and neurodegeneration [2,7]. PLP supports blood sugar control, lowers homocysteine, and acts as an antioxidant, scavenging damaging free radicals [2,10].
A particularly exciting development is the “exercise mimetic” hypothesis: animal and cell studies suggest that PLP can activate muscle protein synthesis pathways (including mTOR and AMPK), similar to the effects of resistance training [3]. In older adults, who often experience sarcopenia (muscle loss) and have lower PLP, this may help preserve muscle mass and strength. Marginal B6 deficiency is surprisingly common in older populations, and supplementation in the 25–50 mg/day range (ideally as PLP) has shown improvements in muscle markers and metabolic health [3,7].
PLP also appears to interact with gut-derived metabolites linked to cardiovascular risk, such as TMAO. B6, especially when combined with vitamin D and other B vitamins, may help lower TMAO levels, suggesting a new gut-microbiome-cardiovascular axis for B6 interventions [7].
The practical takeaway: if you are overweight, sedentary, or aging, and especially if you experience muscle loss or metabolic slowdown, optimizing PLP may yield benefits for blood sugar, cholesterol, inflammation, and muscle preservation. The best-supported strategy is 25–50 mg/day of PLP, taken with food for improved absorption [3,7].
How to Test and Supplement: Mechanisms, Dosage, and Form
Testing for vitamin B6 status should focus on plasma PLP, not just dietary intake or total B6. Plasma PLP captures both intake and how much your body is actually able to use, making it the most sensitive marker for both deficiency and inflammation-driven depletion [6]. Optimal plasma PLP is 30–110 nmol/L, with evidence suggesting >50 nmol/L is best for risk reduction [7,12].
If your PLP is low, the most direct way to raise it is with supplemental pyridoxal-5'-phosphate (PLP), not pyridoxine. PLP bypasses the liver activation step, leading to more reliable increases in blood levels with less variability between individuals [4]. Typical effective dosages are 25–50 mg per day, taken with food to enhance bioavailability and minimize stomach upset [4,7].
Supplementing with PLP at these doses has been shown to raise blood levels to the mid-range of optimal and is safe for long-term use in adults. High doses (>100 mg/day pyridoxine) can cause neuropathy, but this is rare at the dosages supported by studies and is not seen with PLP at typical supplement levels [7].
For certain populations — vegetarians, older adults, those with metabolic syndrome or inflammatory conditions — monitoring and supplementing PLP is particularly important. Plant-based diets often provide B6 as pyridoxine glucoside, which is poorly absorbed, leading to lower PLP despite adequate intake [14]. For these groups, using PLP directly and targeting the optimal blood range is the most evidence-based approach.
What Moves PLP: Factors That Lower or Raise Your B6 Status
Several factors can drive your PLP level down, sometimes dramatically. Chronic inflammation (from obesity, autoimmune disease, or even low-grade gut inflammation) is the single biggest cause of PLP depletion, as inflammatory cells actively consume PLP and increase its breakdown [6,12]. Aging is also associated with lower PLP, in part due to decreased absorption and increased demand [7].
Diet matters, but not as much as once thought. While animal-source B6 is highly bioavailable, plant-source B6 is often bound in a form (pyridoxine glucoside) that is much less absorbable [14]. Alcohol use, certain medications (notably some epilepsy drugs), and oral contraceptives can lower B6 status [5]. On the flip side, regular intake of PLP supplements (25–50 mg/day), especially with a fatty meal, reliably increases blood PLP [4,7].
Intensive exercise, acute infections, and metabolic stress (such as diabetes) can all transiently lower PLP, not by reducing intake, but by rapidly increasing consumption and breakdown [2,6]. This is why tracking PLP over time, not just taking a single measurement, gives the best window into your true status.
If your level is low, the most effective interventions are: (1) supplement with PLP directly (25–50 mg/day); (2) address inflammation with anti-inflammatory diet and lifestyle changes; (3) check for medications or conditions that may be lowering B6 status. Raising PLP is about both intake and reducing unnecessary consumption by the body.
Conclusions
The science on vitamin B6 has evolved dramatically: PLP is not just a marker of dietary adequacy, but a sensitive gauge of your body’s inflammation and metabolic resilience. Low PLP can flag hidden inflammation, signal increased cancer and metabolic risk, and point to nutrient absorption problems — making it a critical, underused test. The most actionable move is to measure your plasma PLP, aim for >50 nmol/L, and supplement with 25–50 mg/day of pyridoxal-5'-phosphate if needed. But always remember: if your PLP stays low despite supplementation, focus on finding and addressing the sources of inflammation. With this biomarker-first approach, you can use vitamin B6 as both a tool for disease prevention and a window into your body’s deeper health.
While observational studies and meta-analyses strongly link PLP with lower cancer and metabolic disease risk, direct interventional trials in humans are still limited. Most supplementation studies use surrogate markers or short-term endpoints. The inflammation-consumption hypothesis is well supported mechanistically, but individual variability in absorption, conversion, and genetic factors may affect PLP response to supplements. Routine PLP testing is not yet standard in most clinical settings. Finally, high-dose B6 (especially pyridoxine >100 mg/day) can cause neuropathy, though this is rare with PLP and within the recommended range.
Track this in your stack
See how vitamin b6 relates to your health goals and monitor changes in your biomarkers over time.
Sources (13)
This article informs how supplementation moves 1 marker.
Each biomarker page clusters supplements, ranges, and the evidence behind every score. Useful when you're starting from a number, not a goal.